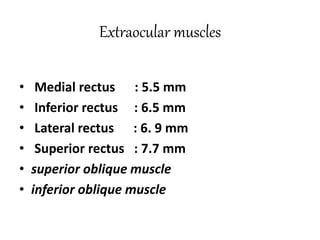
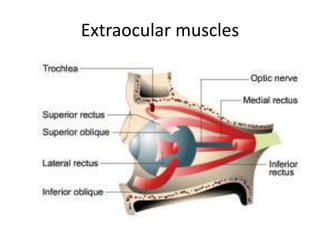
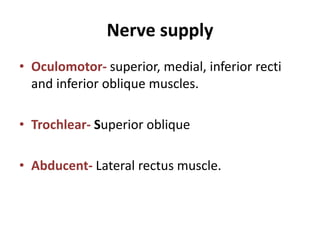
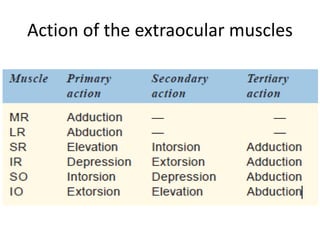
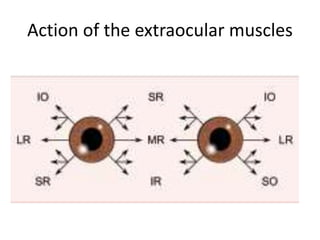
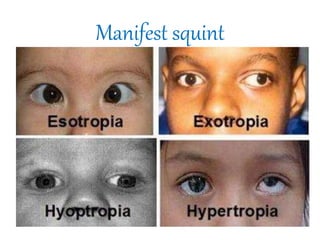
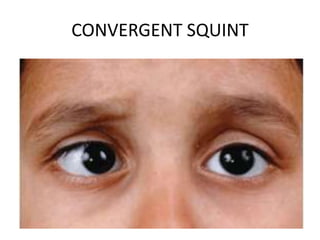
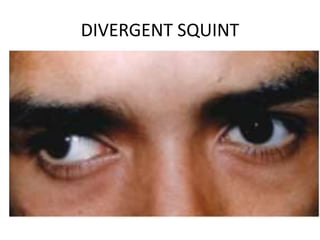
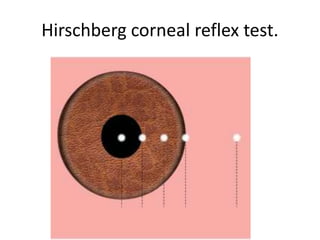
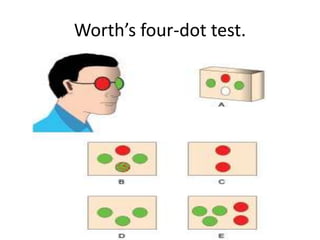
This document discusses strabismus and squint, including the anatomy of the extraocular muscles, ocular motility, binocular vision, heterophoria, manifest squint, evaluation of strabismus cases, and treatment options. It describes the extraocular muscles, types of eye movements, binocular single vision and anomalies. It also defines and classifies heterophoria and manifest squint, discusses their etiology, symptoms, examination and treatment. Evaluation of strabismus cases and different surgical techniques are also outlined.