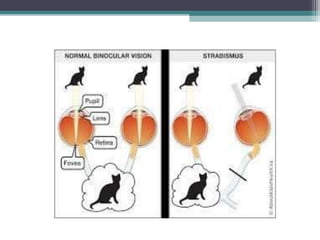
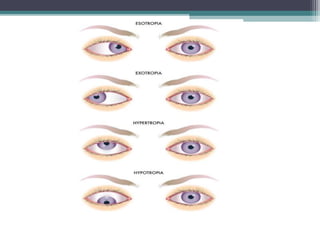
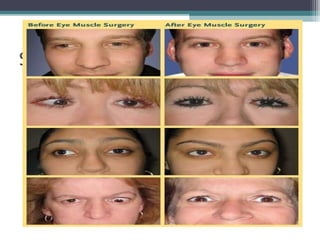
Strabismus, also known as crossed eyes, occurs when the eyes are misaligned and do not look in the same direction. It can be caused by problems with eye muscles, nerves that control the muscles, or the brain's control of eye movement. Treatment may include eyeglasses, eye exercises, eye patching, prisms, vision therapy, eye muscle surgery, or in some cases Botox injections. The goal of treatment is to help the patient achieve normal binocular vision and alignment of the eyes in all directions of gaze.










































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)










