Downloaded 47 times




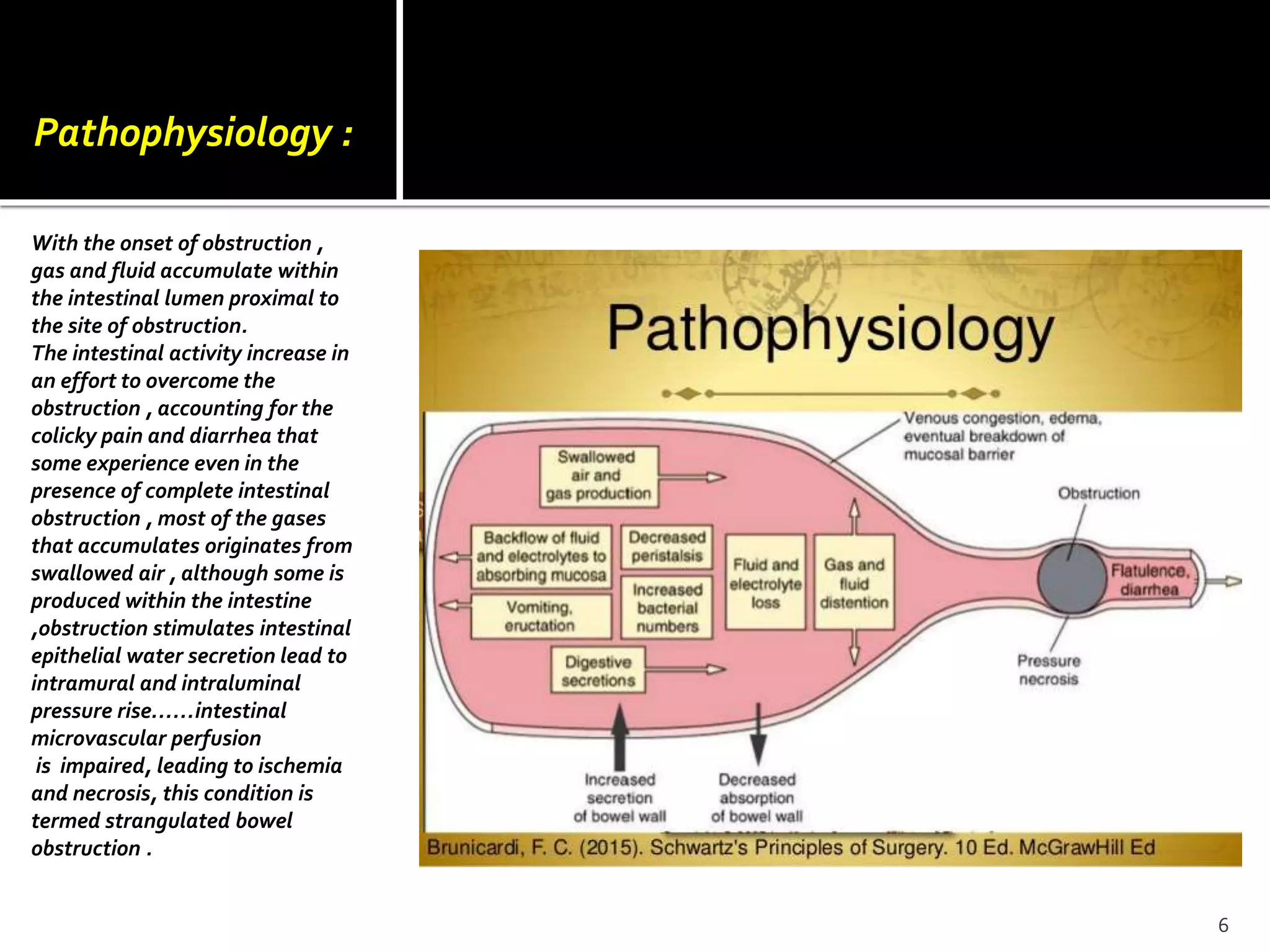

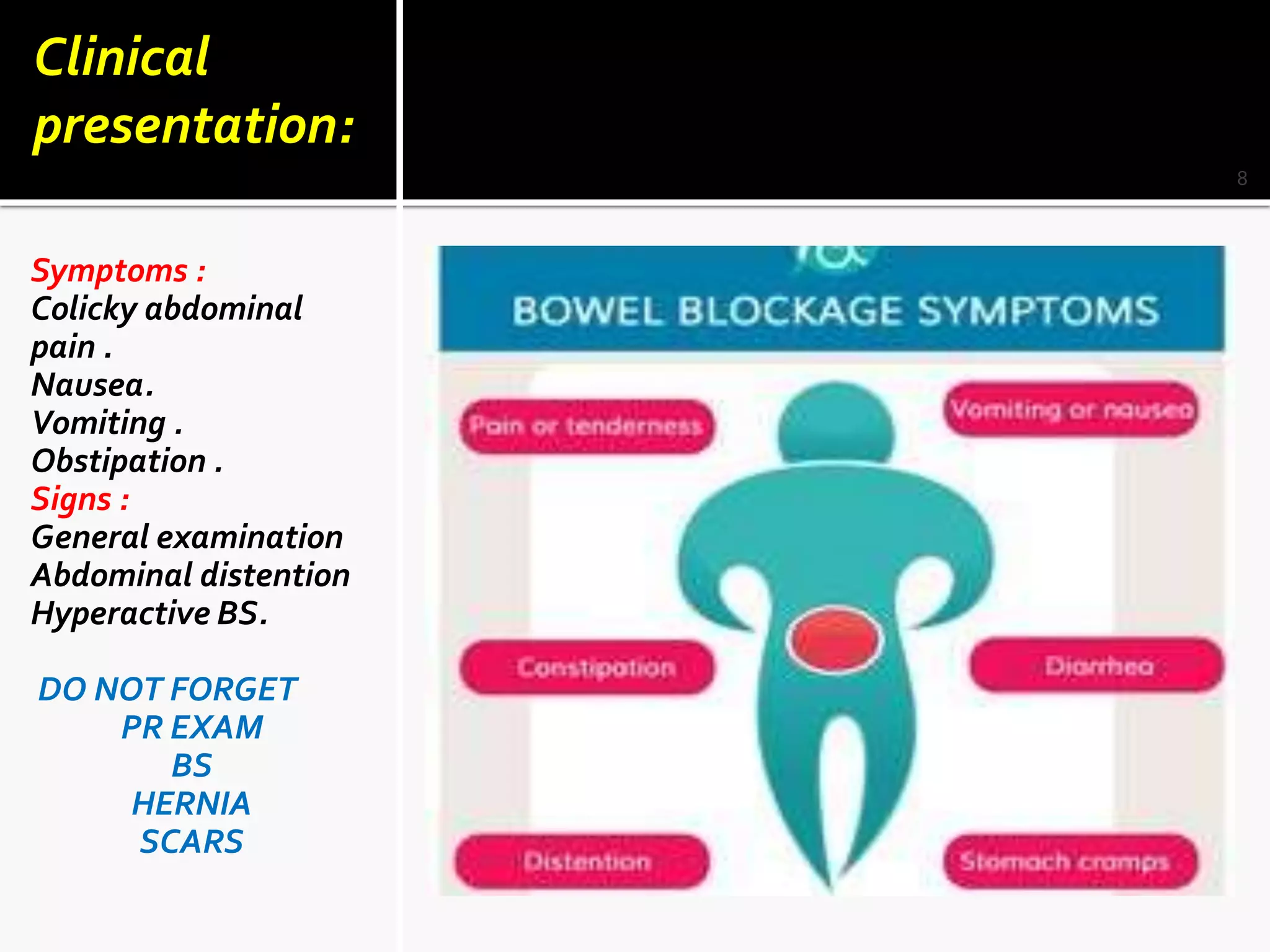



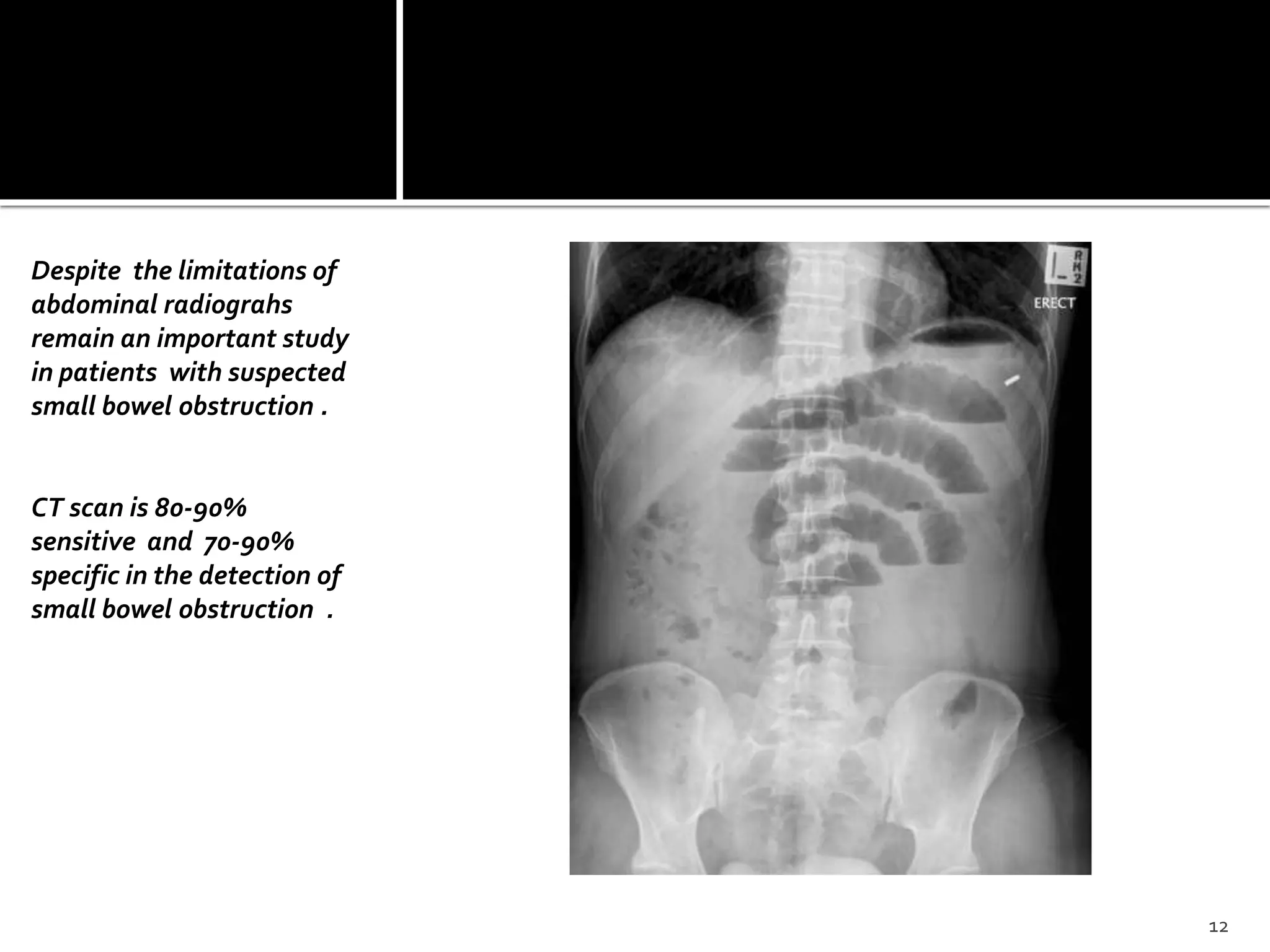





This document discusses small bowel obstruction, including its pathophysiology, clinical presentation, diagnosis, management, and prevention. The pathophysiology section explains how obstruction leads to accumulation of gas and fluid in the bowel above the site of obstruction. The clinical presentation section outlines common symptoms like colicky abdominal pain and nausea/vomiting, as well as signs seen on examination. Diagnosis involves distinguishing mechanical obstruction from ileus, determining the etiology, and discriminating between partial and complete or simple versus strangulating obstruction, often using radiological exams. Management depends on whether the obstruction is simple or strangulated. With conservative treatment, the majority of patients with adhesive small bowel obstruction are readmitted in less than 20% of cases over 5



































































