Download to read offline
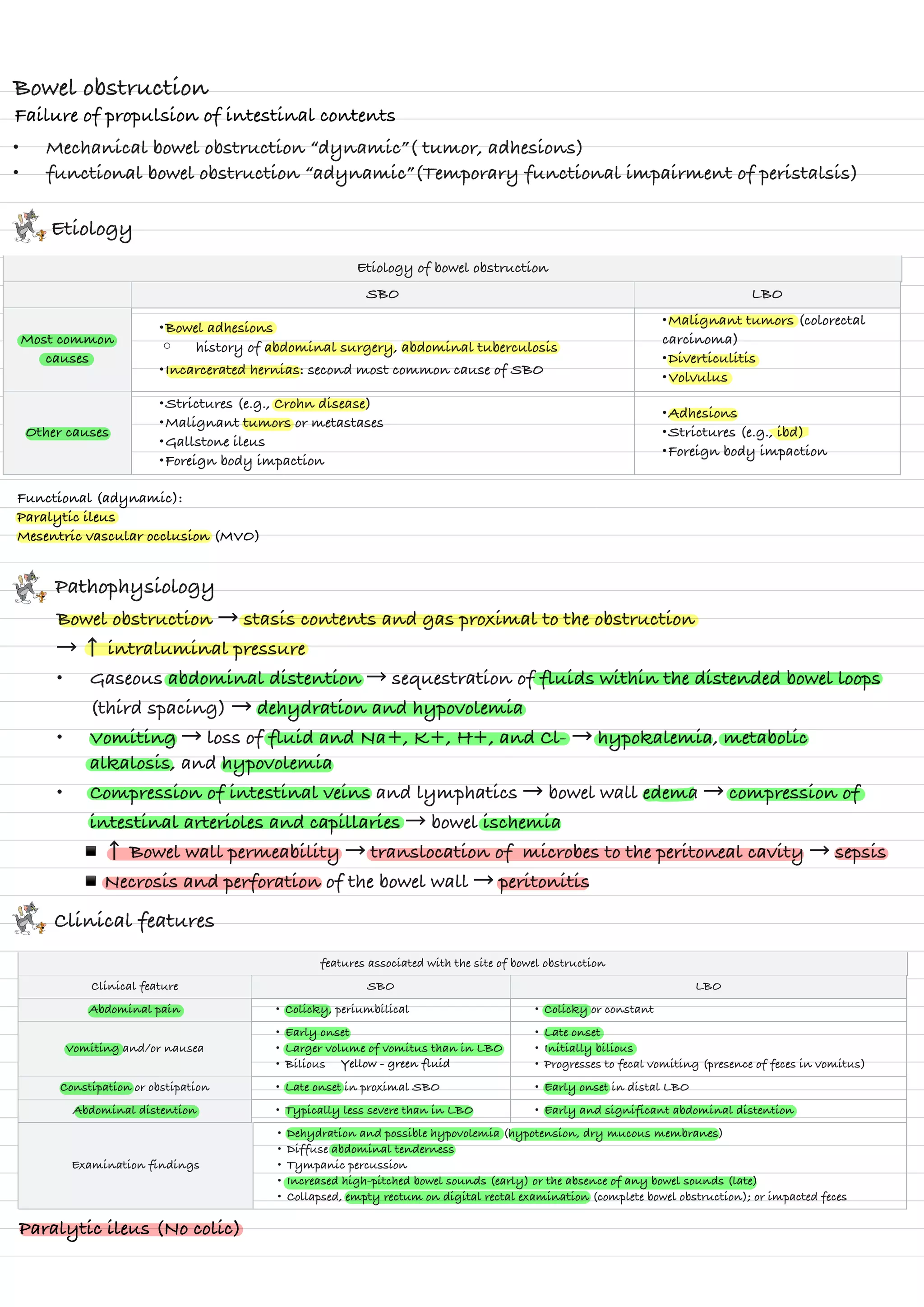

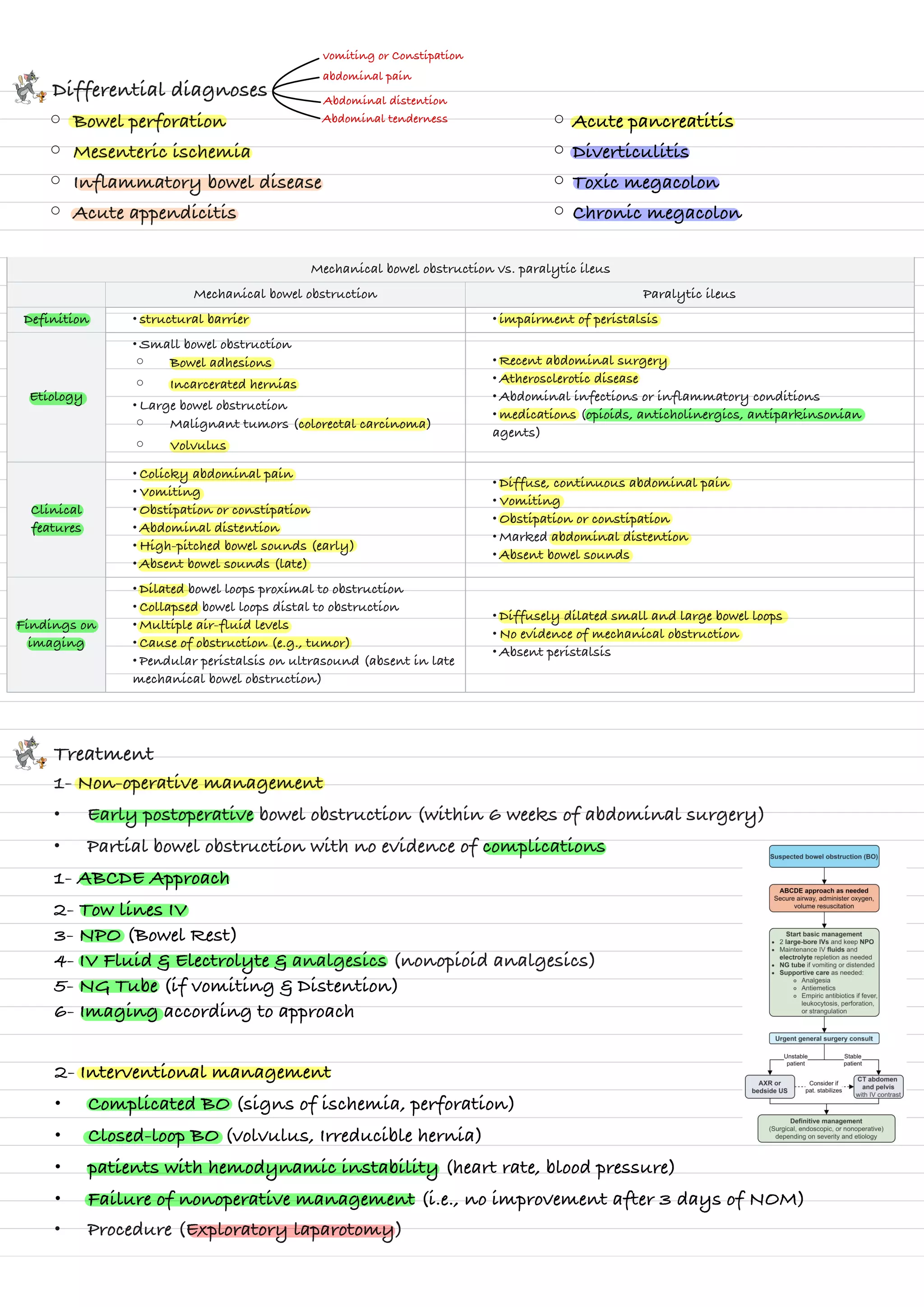

Mechanical bowel obstruction is caused by structural barriers like adhesions or tumors blocking intestinal contents. The most common causes are abdominal adhesions, hernias, and colorectal cancer. This leads to a build up of gas and fluids proximal to the obstruction, causing pain, vomiting, distention and potentially ischemia if not resolved. Paralytic ileus is a functional obstruction caused by impaired peristalsis due to factors like surgery or infection. Treatment involves decompression with NG tubes, IV fluids and electrolytes, and surgery if signs of complication or failure to improve. Surgical intervention aims to release the obstruction and prevent complications.



































































