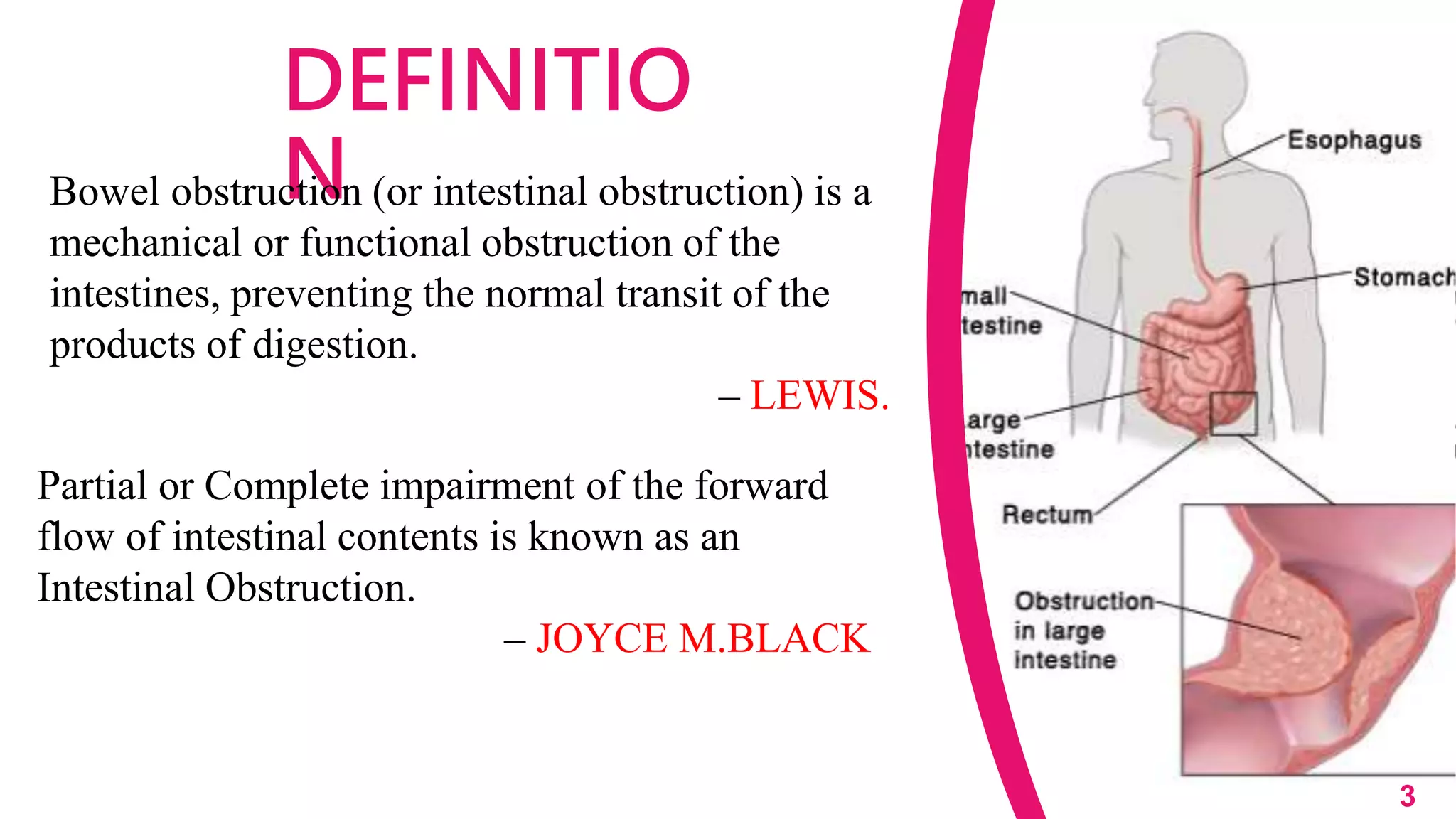





1. Bowel obstruction occurs when the bowel becomes blocked, preventing food and liquids from passing through the intestines. This can affect either the small or large intestine. 2. There are different types of bowel obstruction including small or large intestine obstruction, partial or complete obstruction, and mechanical or functional obstruction. 3. Symptoms of bowel obstruction include abdominal pain, bloating, vomiting, constipation, and loss of appetite. Diagnosis involves imaging tests and physical examination to locate the blockage. 4. Treatment depends on the severity and includes managing symptoms, surgery to remove or bypass the blockage, and nursing care during recovery. Complications can include infection, sepsis, and short bowel syndrome.























































































