Downloaded 343 times

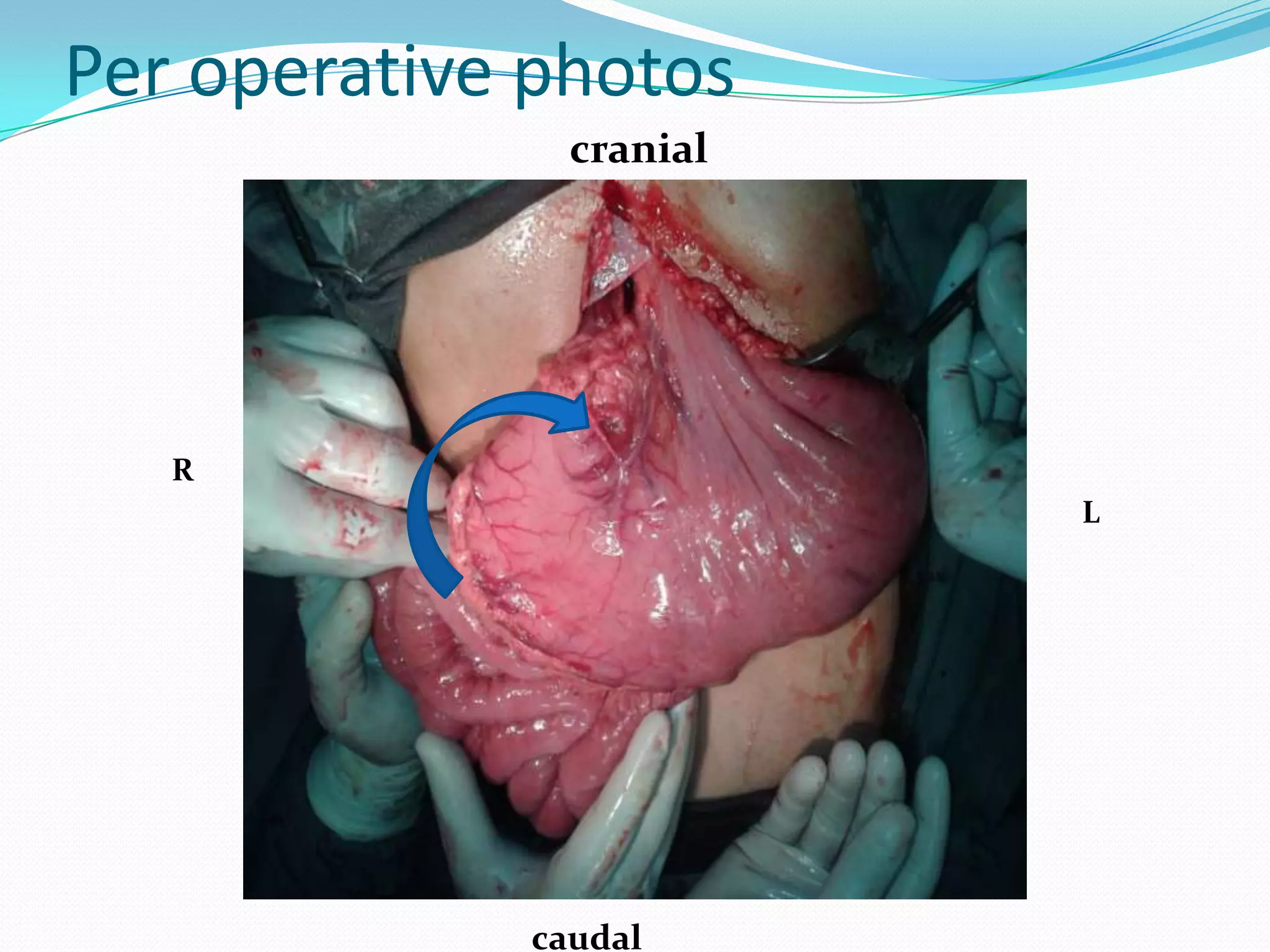


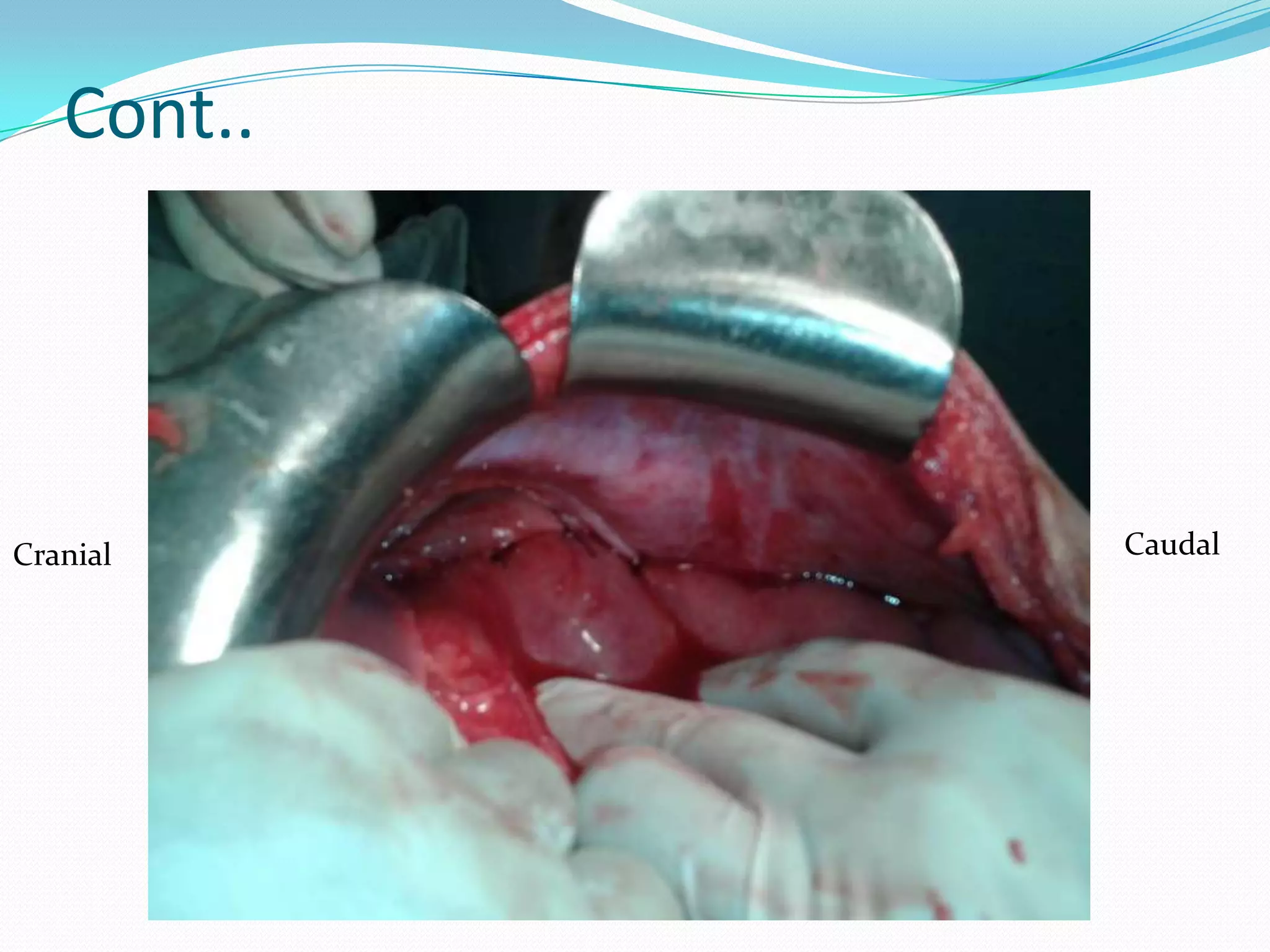
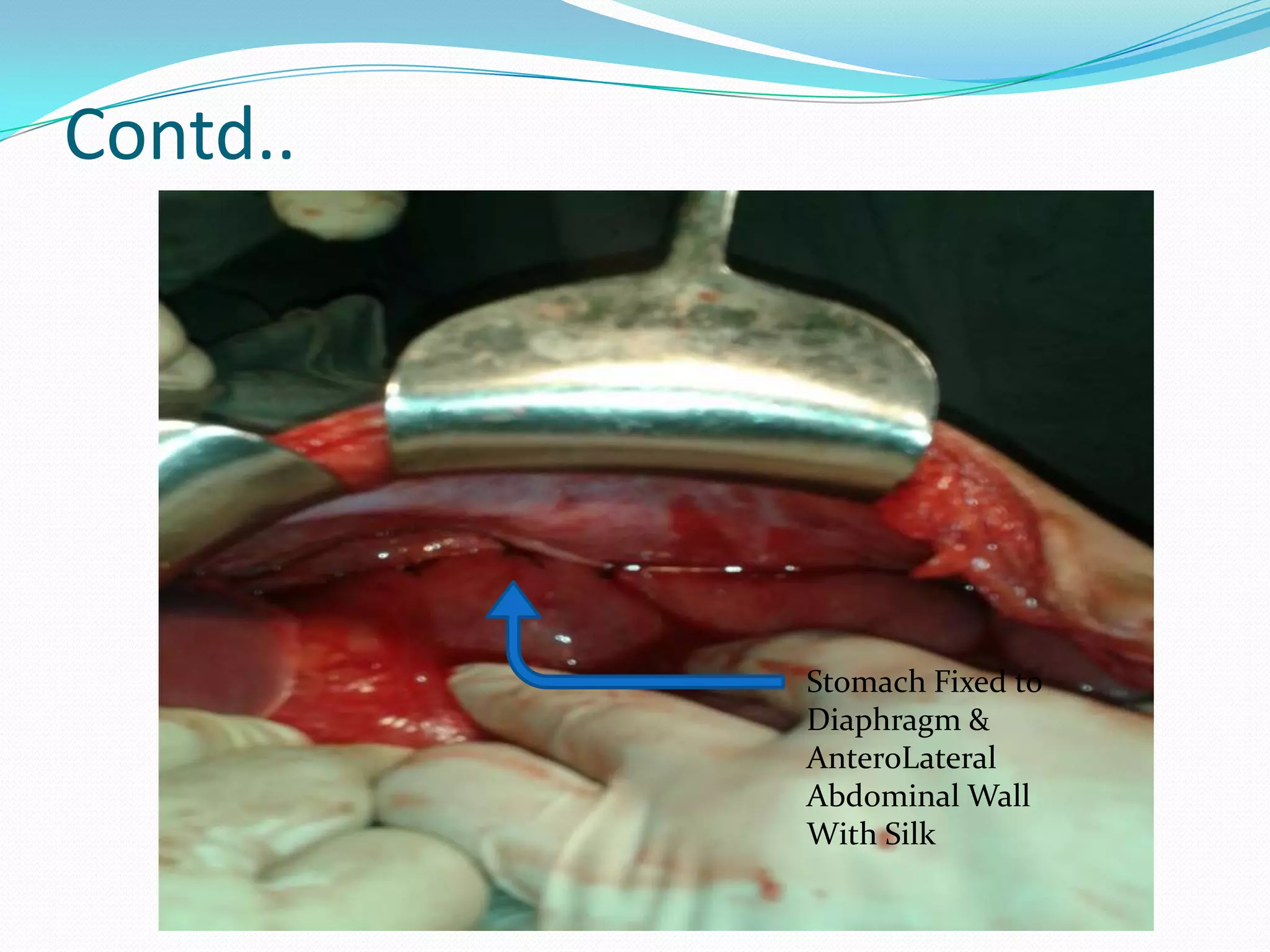
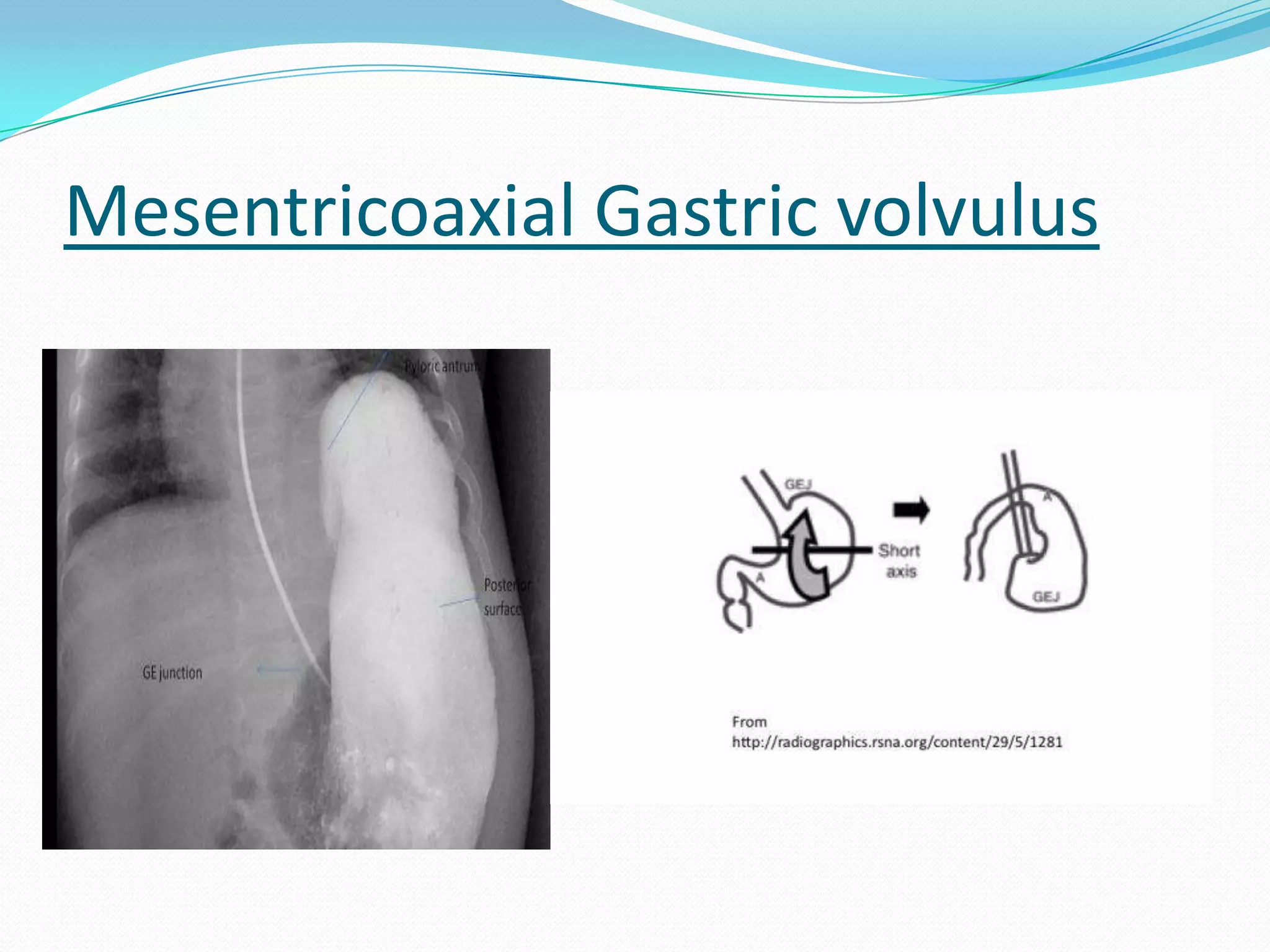
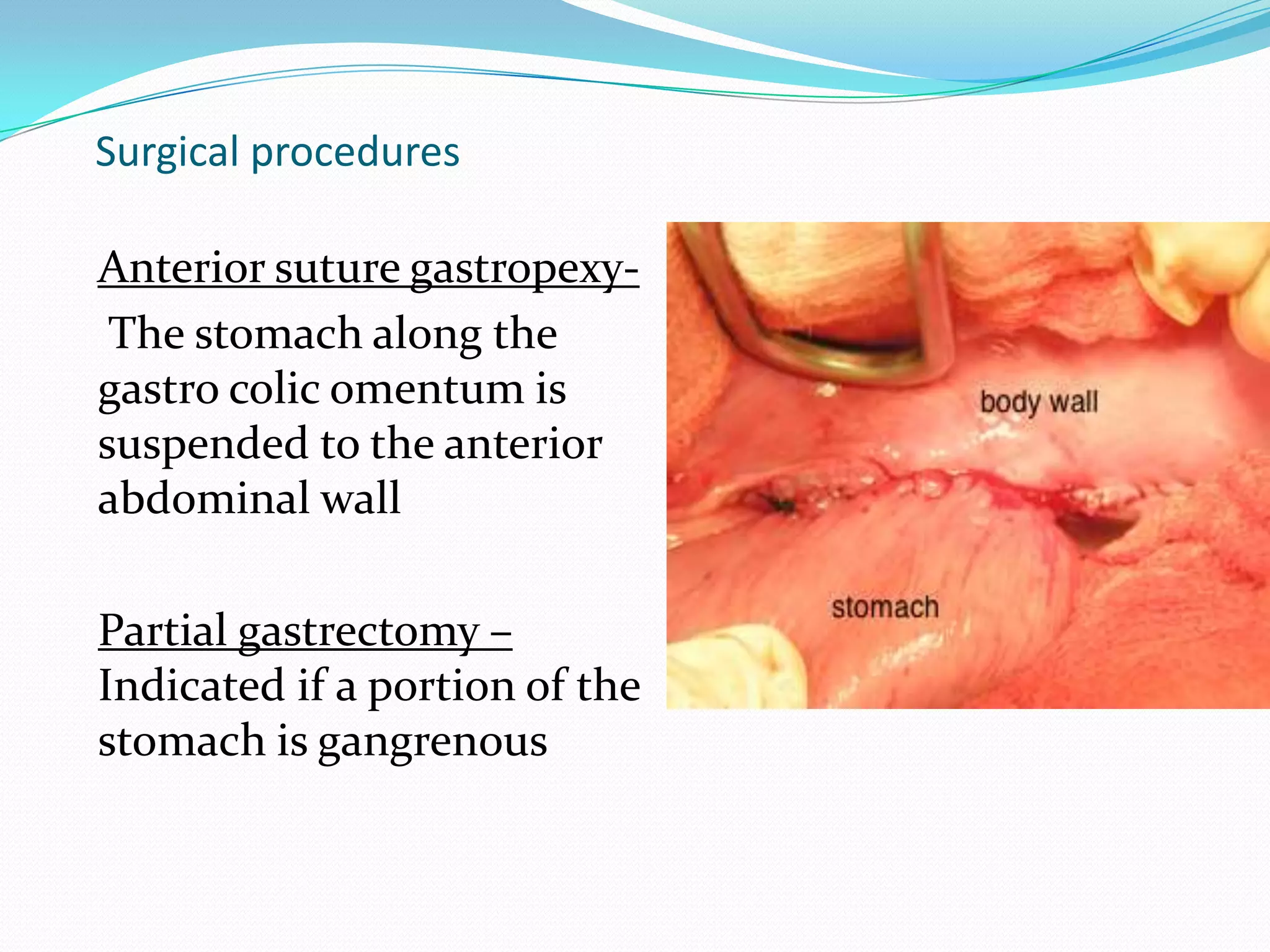
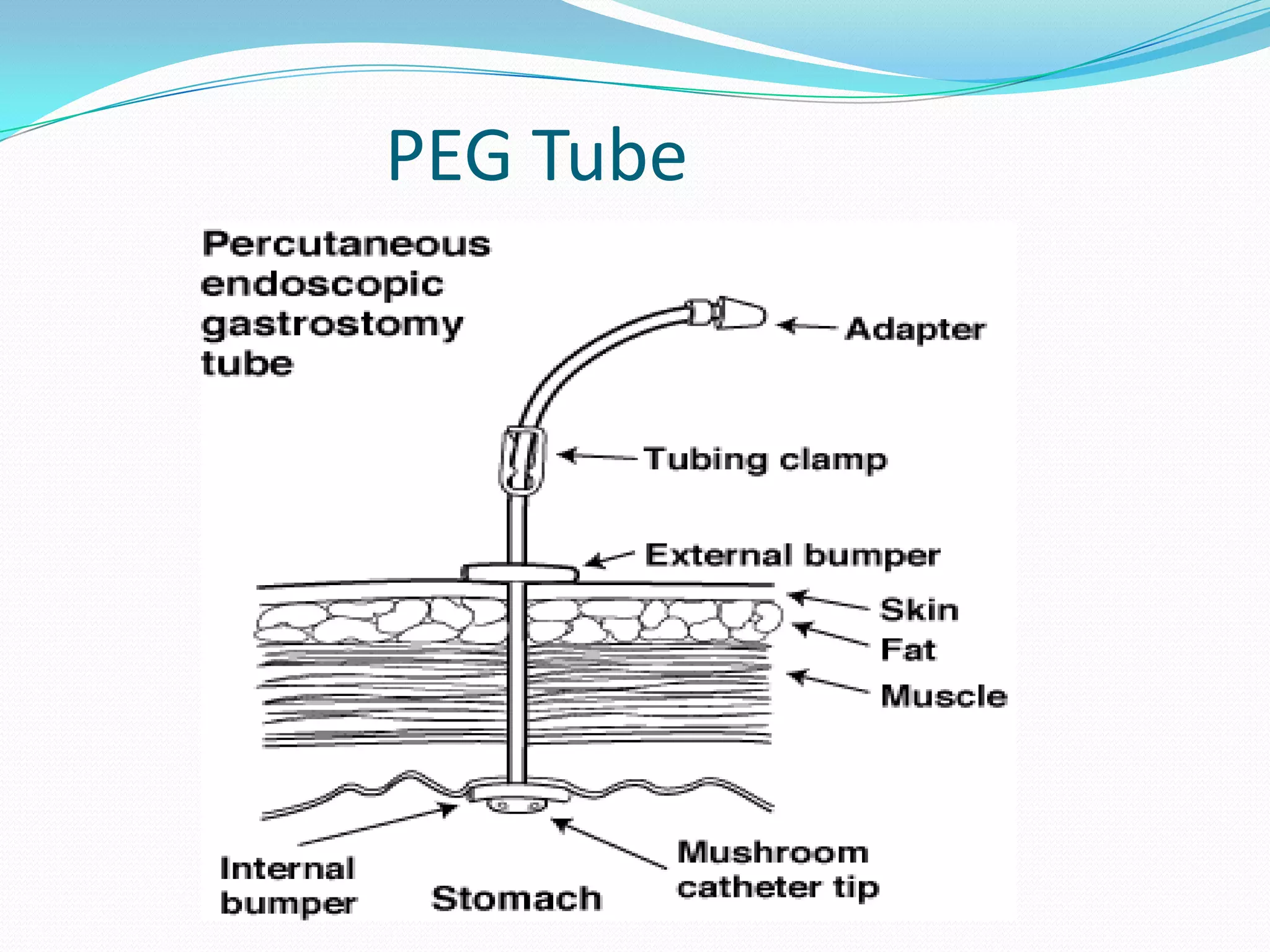


Bhori Singh, a 45-year-old male, presented with abdominal pain, distension and inability to pass flatus or stool for the past few days. Examination and investigations revealed acute intestinal obstruction likely due to gastric volvulus or perforation peritonitis. He underwent an exploratory laparotomy with gastropexy where gastric volvulus was found and repaired by suturing the stomach to the abdominal wall. Post-operatively, he recovered well and was discharged on the 8th day. Gastric volvulus is the twisting of the stomach and can be acute or chronic. Treatment involves endoscopic or surgical reduction and fixation of the stomach to prevent recurrence.















































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)


















