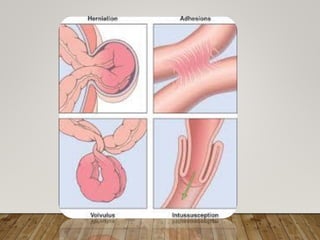
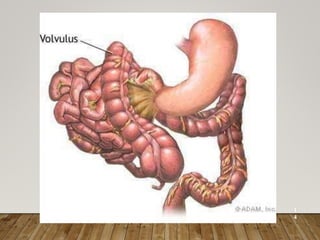
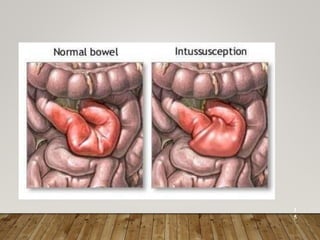
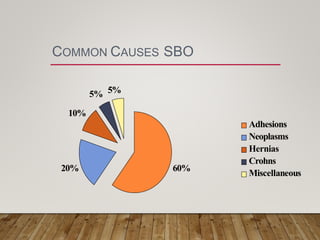
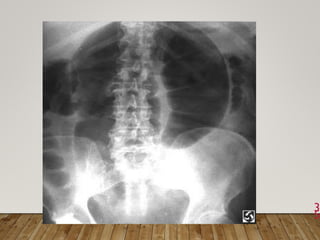
The document discusses intestinal obstruction, defining it as an interruption of normal passage of intestinal contents and classifying it into dynamic and adynamic types, with various causes including adhesions, hernias, and tumors. It details symptoms, diagnostic approaches, and management strategies, highlighting the importance of identifying the level of obstruction, presence of strangulation, and dehydration status. Non-operative management may involve gastrointestinal decompression, while operative approaches are typically necessary for complicated cases.