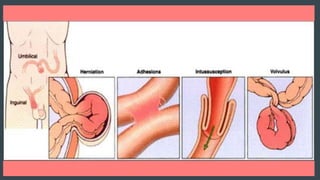
This document discusses intestinal obstruction, including its classification, causes, pathophysiology, diagnosis, and treatment. Intestinal obstruction can be dynamic, involving peristalsis against a blockage, or adynamic with no mechanical blockage. Causes include adhesions, hernias, tumors, and inflammation. Diagnosis involves history, exam, and imaging tests. Treatment depends on severity but generally involves resuscitation, decompression, and surgery if conservative measures fail or for strangulated obstructions.


![CLASSIFICATION
Dynamic/ Adynamic
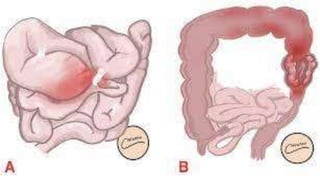
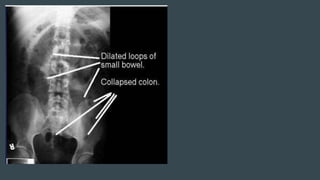
Small bowel obstruction [ high or low ]
Large bowel obstruction
Acute, Chronic, Acute on chronic ,Subacute
Simple
Strangulated
Closed loop obstruction](https://image.slidesharecdn.com/intestinalobstruction-230411065427-f0d7576b/85/INTESTINAL-OBSTRUCTION-pptx-3-320.jpg)