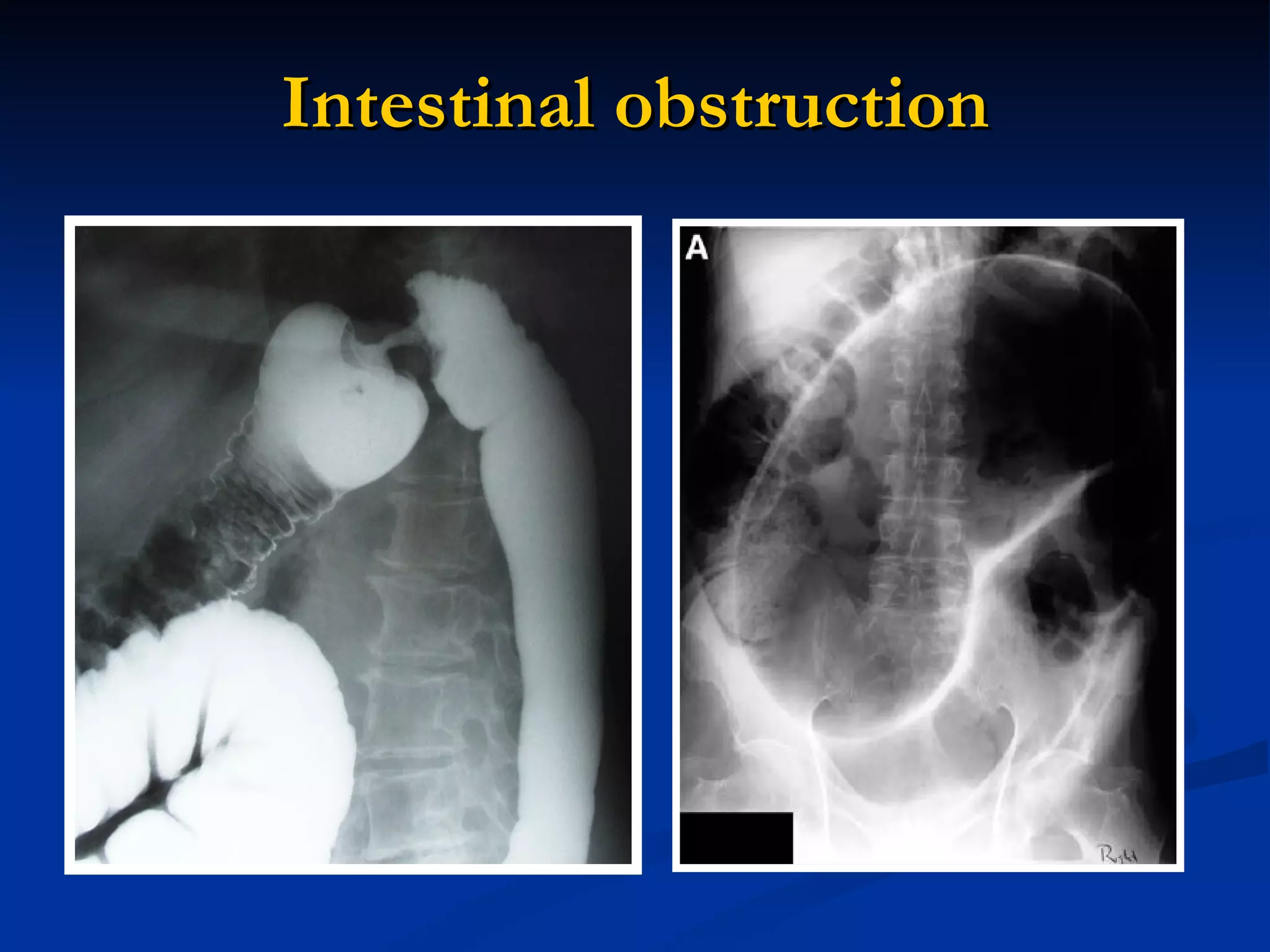
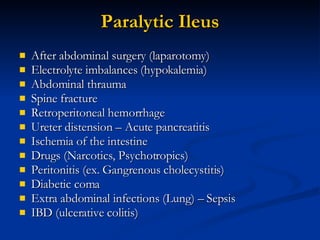
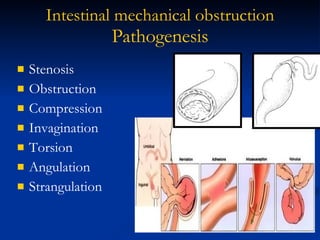
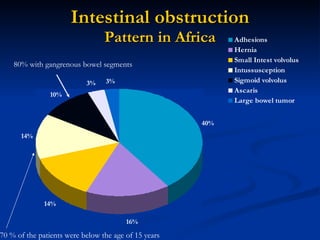
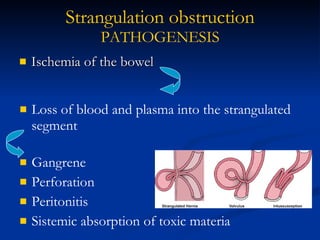
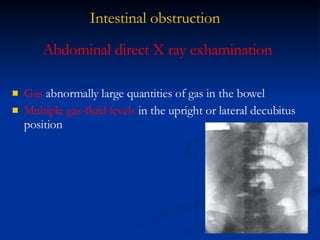
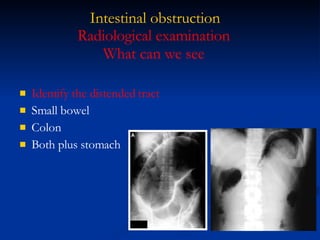
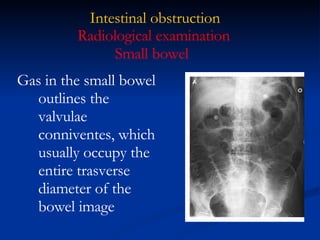
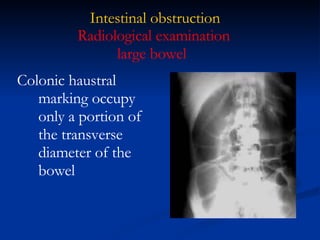
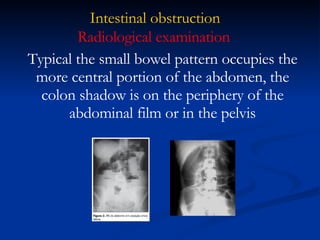
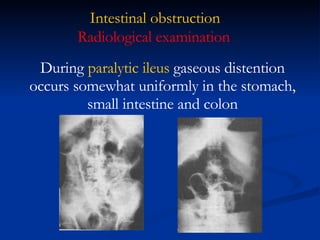
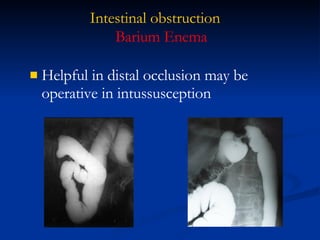
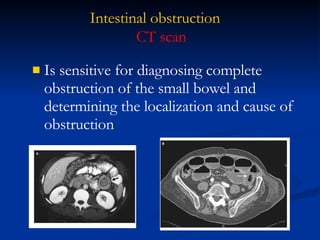
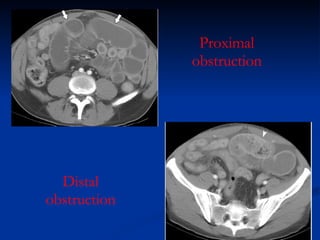
This document discusses intestinal obstruction, including its causes, symptoms, diagnosis, and treatment. It describes two main types - mechanical obstruction caused by physical blockage, and paralytic ileus caused by loss of intestinal motility. Common symptoms are abdominal pain, vomiting, constipation, and distension. Diagnosis involves abdominal x-rays to detect gas patterns and fluid levels. Treatment focuses on fluid resuscitation, decompression with NG tubes, and timely surgery to relieve blockages and prevent complications like strangulation.