Downloaded 134 times

















![Volvulus neonatorium
Abdominal radiograph
Evidence of duodenal obstruction
Later intestinal strangulation progress abdomen
relatively gasless
Reduce volvulus at operation [decompression using
needle]
Caecopexy (fixation of caecum to right iliac fossa)
Caecostomy
If ischaemic or gangrenous caecum right
hemicolectomy](https://image.slidesharecdn.com/intestinalobstruction1-190712154223/75/Intestinal-obstruction-24-2048.jpg)
![A. Management of Caecal
Volvulus
Reduce volvulus at operation [decompression using
needle]
Caecopexy (fixation of caecum to right iliac fossa)
Caecostomy
If ischaemic or gangrenous caecum right
hemicolectomy](https://image.slidesharecdn.com/intestinalobstruction1-190712154223/75/Intestinal-obstruction-25-2048.jpg)








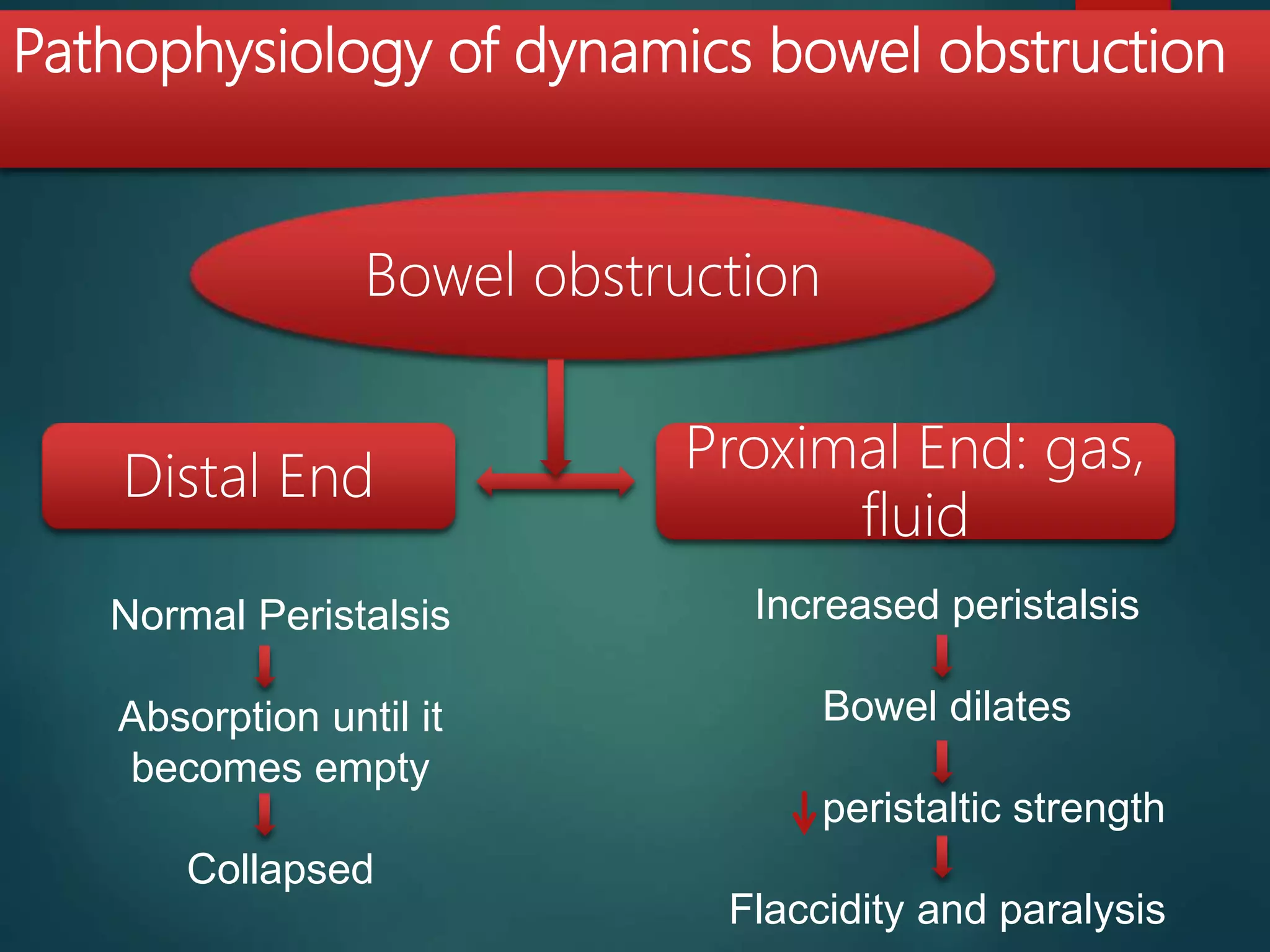
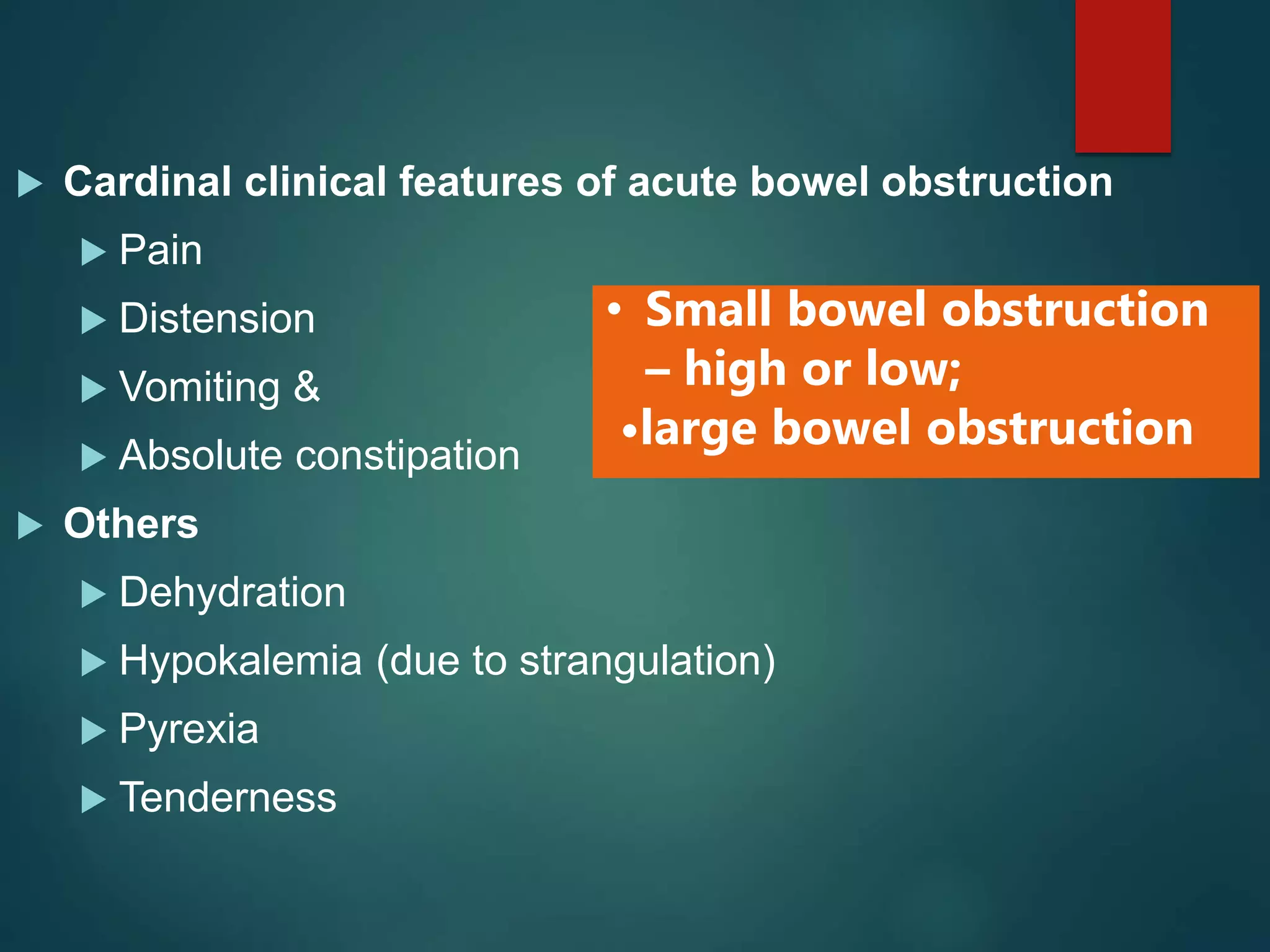
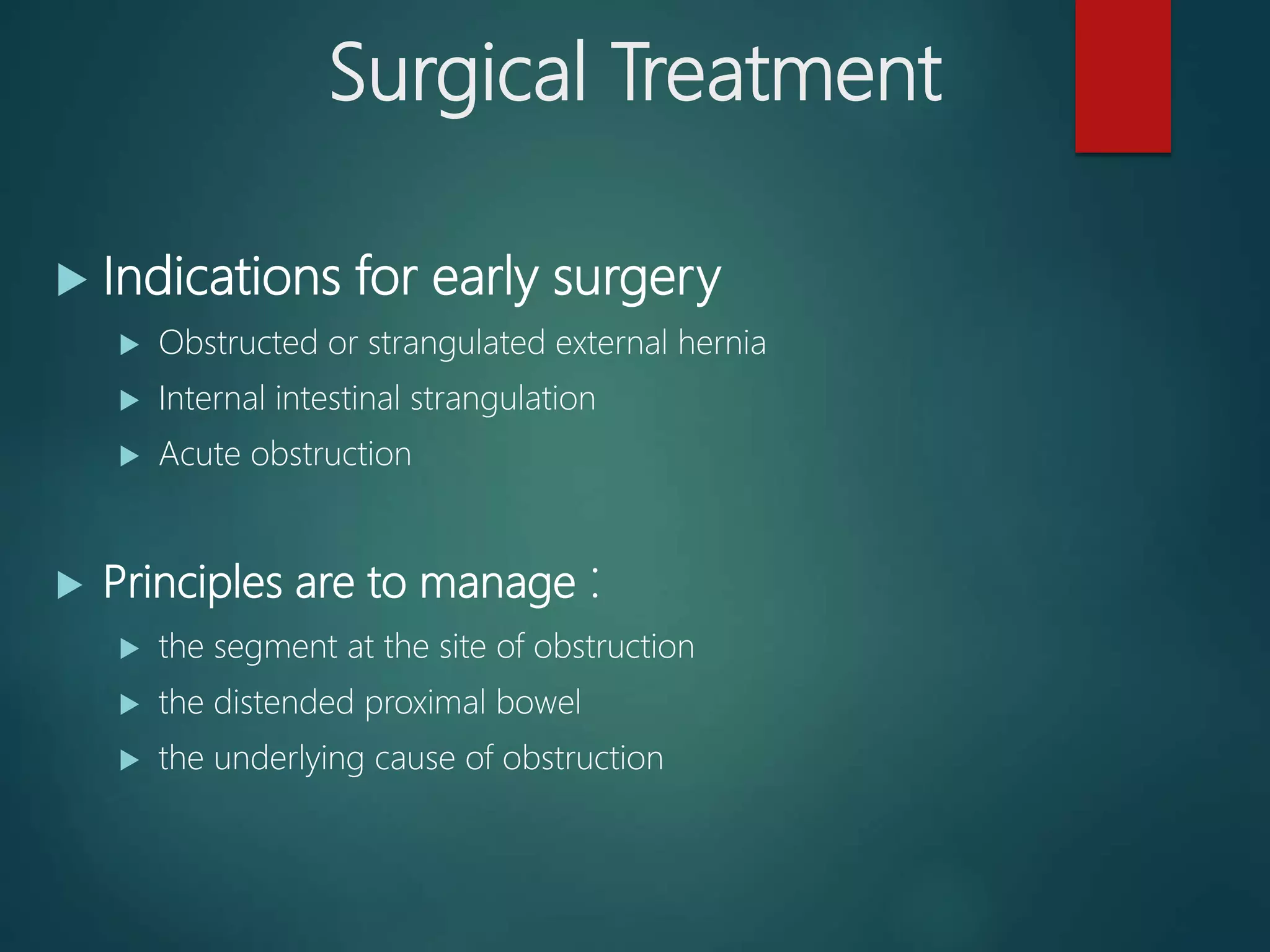
This document discusses various causes and types of intestinal obstruction, including their presentation, diagnosis and management. It covers mechanical obstructions caused by adhesions, hernias, volvulus and intussusception. It also discusses paralytic ileus and pseudo-obstruction which are adynamic obstructions without a mechanical cause. The management involves supportive care, surgical correction of the underlying cause, and resection of non-viable intestine. Early diagnosis and treatment are important to prevent complications like strangulation.























































































