2
Introduction
The earliestresponse of the proximal
gut to obstruction is
Increase bowel wall contractility to
overcome the blockage
7/14/2025
3.
3
Cont…
Intra-abdominal adhesionsrelated to prior
abdominal surgery
Account for up to 75% of cases of small
bowel obstruction.
Over 300,000 patients are estimated to
undergo surgery to treat adhesion-induced
SBO in USA
7/14/2025
4.
4
Epidemiology
Small bowelobstruction is a common surgical problem
and
Accounts for as many as 400,000 hospital admissions
annually, and
30-40% of these patients will require operative
exploration
Mechanical small bowel obstruction is the most
frequently encountered surgical disorder of the small
intestine
7/14/2025
5.
5
Etiologies
a. Intraluminal (e.g.,foreign bodies,
gallstones, or meconium)
b. Intramural (e.g., tumors, Crohn’s disease–
associated inflammatory strictures)
c. Extrinsic (e.g., adhesions, hernias, or
carcinomatosis)
7/14/2025
6.
6
Cont…
Less prevalentetiologies for small bowel
obstruction include
Hernias
Malignant bowel obstruction
Crohn’s disease
The frequency with which obstruction related to
these conditions is encountered varies according
to the patient population and practice setting
7/14/2025
7.
7
Cont…
Cancer-related smallbowel obstructions are
commonly due to
Extrinsic compression or
Invasion by advanced malignancies arising in organs
other than the small bowel
Few are due to primary small bowel tumors
The most commonly encountered etiologies of
SBO
7/14/2025
10
Cont…
Congenital abnormalitiescapable of
causing small bowel obstruction usually
become evident during childhood
They sometimes elude detection and are
diagnosed for the first time in adult
patients presenting with abdominal
symptoms
7/14/2025
11.
11
Cont…
Intestinal malrotationand midgut
volvulus should not be forgotten
When considering the differential diagnosis
of adult patients with SBO
Especially those without a history of
prior abdominal surgery
7/14/2025
12.
12
Cont…
A rareetiology of obstruction is the superior
mesenteric artery syndrome
Characterized by compression of the third portion
of the duodenum by the SMA
As it crosses over this portion of the duodenum
This should be considered in young asthenic
individuals
Who have chronic symptoms suggestive of proximal
small bowel obstruction
7/14/2025
14
Pathophysiology
With onsetof obstruction, gas and fluid
accumulate within the intestinal lumen
proximal to the site of obstruction
The intestinal activity increases to overcome
the obstruction
Accounting for the colicky pain and the diarrhea
that some experience even in the presence of
complete bowel obstruction
7/14/2025
15.
15
Cont…
Most ofthe gas that accumulates originates
from swallowed air
Although some is produced within the intestine
The fluid consists of swallowed liquids and
gastrointestinal secretions
Obstruction stimulates intestinal epithelial
water secretion
7/14/2025
16.
16
Cont…
Dilatation andlack of contractility
may allow water and electrolytes to
accumulate proximal to the obstruction
Significant third space losses in
addition to vomiting may result in
Marked dehydration and hypovolemia
7/14/2025
17.
17
Cont…
Metabolic derangementmay be significant,
and depends on the level of the obstruction
Proximal obstruction may result in
Hypochloremia
hypokalemia, and
metabolic alkalosis
Concurrent, persistent vomiting can exacerbate these
alterations
7/14/2025
18.
18
Cont…
Obstruction ofthe distal small bowel
results in a larger capacitance effect
with enhanced volume loss
Electrolyte disturbances may be
somewhat less severe
However, significant hypovolemia and
Even renal damage can occur
7/14/2025
19.
19
Cont…
Obstruction provokesa profound
change in the flora of the small intestine
With stasis permitting
Overgrowth of the few native species
Reverse peristalsis from the colonic
microbiota
7/14/2025
20.
20
Cont…
With obstruction,the luminal flora of
the small bowel, which is usually sterile,
changes and
A variety of organisms have been
cultured from the contents
Translocation of these bacteria to
regional lymph nodes has been
7/14/2025
21.
21
Cont…
These aremost commonly
Escherichia coli
Streptococcus
Faecalis
Klebsiella species
Overgrowth can occur rapidly
7/14/2025
22.
22
Cont…
Even priorto frank perforation with gross
contamination
There is evidence that bacteria can translocate
through the intestinal wall and
May well contribute to a deteriorating sepsis
picture
If the treatment of initial obstruction is delayed
7/14/2025
23.
23
Cont…
With ongoinggas and fluid
accumulation, the bowel distends and
intraluminal and intramural pressures
rise
The intestinal motility is eventually
reduced with fewer contractions
7/14/2025
24.
24
Cont…
If obstructionis not relieved and these
processes continue volume loss and abdominal
distention will result in
Decreased venous return
Diapragmatic elevation
Compromised ventilation
All of which will exacerbate the symptoms of an
acute abdomen
7/14/2025
25.
25
Cont…
If theintramural pressure becomes high
enough
Intestinal microvascular perfusion is
impaired leading to intestinal ischemia,
and, ultimately, necrosis
This condition is termed strangulated
bowel obstruction
7/14/2025
26.
26
Cont…
With partialSBO, only a portion of the
intestinal lumen is occluded
Allowing passage of some gas and fluid
The progression of pathophysiologic
events occur more slowly than with
complete SBO
Development of strangulation is less likely
7/14/2025
27.
27
Cont…
A particularlydangerous form of bowel obstruction is
closed loop obstruction
In which a segment of intestine is obstructed both
proximally and distally (volvulus)
The accumulating gas and fluid cannot escape either
proximally or distally from the obstructed segment
This leading to a rapid rise in luminal pressure and a
rapid progression to strangulation
7/14/2025
28.
28
CLINICAL PRESENTATION ANDDIAGNOSIS
CLINICAL FINDINGS
The symptoms of small bowel obstruction are
Colicky abdominal pain
Nausea
Vomiting
Obstipation
Vomiting is a more prominent symptom with
proximal obstructions than distal
7/14/2025
29.
29
Cont…
Character ofvomitus is important as with
bacterial overgrowth
The vomitus is more feculent, suggesting a more
established obstruction
Continued passage of flatus and/or stool beyond
6-12 hrs after onset of symptoms is characteristic
of partial rather than complete obstruction
7/14/2025
30.
30
Cont…
The signsof SBO include abdominal
distention
Which is most pronounced, If the site of
obstruction is in the distal ileum and
May be absent if the site of obstruction is
in the proximal small intestine
7/14/2025
31.
31
Cont…
Bowel sounds
Maybe hyperactive initially
In late stages of bowel obstruction, minimal bowel
sounds may be heard
Laboratory findings reflect intravascular volume
depletion
Hemoconcentration and electrolyte abnormalities
Mild leukocytosis is common
7/14/2025
32.
32
Cont…
Features ofstrangulated obstruction
include
Abdominal pain often disproportionate to
the degree of abdominal findings
Suggestive of intestinal ischemia
7/14/2025
33.
33
Cont…
Patients oftenhave
Tachycardia
Localized abdominal tenderness
Fever
Marked leukocytosis
Acidosis
Any of these findings should alert the clinician to the
possibility of strangulation and the need for early
surgical intervention
7/14/2025
34.
34
Cont…
A septicpicture raises the more ominous
diagnosis of strangulated bowel or leak
Both result in a more seriously ill patient whose
complication rate and
Mortality can be worsened by a delay in diagnosis
Bowel wall integrity can be compromised by a
folding or knuckling of the bowel from adhesion
or hernia
7/14/2025
35.
35
Cont…
Additionally, patientsprone to arterial
emboli can have mesenteric ischemia
Present with an ileus/obstruction picture
In patients with strangulation or leakage
The WBC can be elevated along with
serum lactate levels
7/14/2025
36.
36
Cont…
Abdominal tendernessand rebound are usually
more pronounced than in simple mechanical
obstruction
Bowel sounds are usually diminished or absent
In all cases where obstruction or strangulation
is suspected, a rectal exam must be performed
7/14/2025
37.
37
Diagnosis
The diagnosticevaluation should focus on the
following goals:
a. Distinguish mechanical obstruction from ileus
b. Determine the etiology of the obstruction
c. Discriminate partial from complete obstruction,
and
d. Discriminate simple from strangulating
obstruction
7/14/2025
38.
38
Cont…
The radiologicassessment of these patients must
focus on several important questions:
1) Is the small bowel obstructed
2) What is the severity of the bowel obstruction?
3) Where is the obstruction located?
4) What is the etiology of the obstruction?
5) Is there a closed-loop obstruction?
6) Is bowel ischemia or strangulation present?17
7/14/2025
39.
39
Cont…
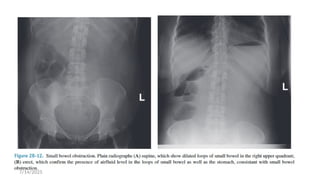
The diagnosisof SBO is usually confirmed with
radiographic examination
The abdominal series consists of
I. A radiograph of the abdomen with the patient in a
supine position
II. A radiograph of the abdomen with the patient in an
upright position
III. A radiograph of the chest with the patient in an upright
position
7/14/2025
40.
40
Cont…
The findingmost specific for SBO is the
triad of
Dilated small bowel loops (>3 cm in
diameter)
Air-fluid levels seen on upright films, and
A paucity of air in the colon
7/14/2025
41.
41
Cont…
The sensitivityof abdominal radiographs in
the detection of small bowel obstruction
ranges from 70-80%
Specificity is low because ileus and colonic
obstruction can be associated with findings
That mimic those observed with small
bowel obstruction
7/14/2025
42.
42
Cont…
False-negative findingson radiographs
can result when
The site of obstruction is in the proximal
small bowel
The bowel lumen is filled with fluid but no gas
There by preventing visualization of air-fluid
levels or bowel distention
7/14/2025
43.
43
Cont…
The lattersituation is associated with
closed-loop obstruction
Despite these limitations
Abdominal radiographs remain an
important study in pts with suspected small
bowel obstruction because of their
widespread availability and low cost
7/14/2025
46
Cont…
CT scanningis becoming increasingly
the imaging test of choice for pts with
SBO
It is ideally done with oral contrast
CT is 80-90% sensitive and 70-90%
specific in the detection SBO
7/14/2025
47.
47
Cont…
The findingsof SBO include a
Discrete transition zone with dilation of
bowel proximally
Decompression of bowel distally
Intraluminal contrast that does not pass
beyond the transition zone
Colon containing little gas or fluid
7/14/2025
50
Cont…
CT scanningmay also provide evidence for the
presence of closed loop obstruction and strangulation
Closed-loop obstruction is suggested by the presence
of a
U-shaped or C-shaped dilated bowel loop associated with
a radial distribution of mesenteric vessels converging
toward a torsion point
7/14/2025
51.
51
Cont…
Strangulation issuggested by
Thickening of the bowel wall
Pneumatosis intestinalis (air in the bowel wall)
Portal venous gas
Mesenteric haziness
Poor uptake of intravenous contrast into the
wall of the affected bowel
7/14/2025
52.
52
Cont…
CT scanningalso offers a global evaluation of
the abdomen and
May therefore reveal the etiology of obstruction
This feature is important in the acute setting
When intestinal obstruction represents only one of
many diagnoses in patients presenting with acute
abdominal conditions
7/14/2025
53.
53
Cont…
The CTscan is usually performed after
administration of oral water-soluble contrast or
diluted barium
The water-soluble contrast has been shown to have
prognostic and therapeutic values too
Several studies and several subsequent meta-
analysis have shown that water-soluble contrast
could in fact have therapeutic and prognostic value
7/14/2025
54.
54
Cont…
The appearanceof the contrast in the
colon within 24 hrs of administration is
predictive of nonsurgical resolution of
bowel obstruction
Sensitivity of 92% and a specificity of 93%
7/14/2025
55.
55
Cont…
A limitationof CT scanning is its low sensitivity
(<50%) in the detection of low-grade or partial
small bowel obstruction
A subtle transition zone may be difficult to identify in
the axial images obtained during CT scanning
In such cases, contrast examinations of the
small bowel, either small bowel series (small
bowel follow-through) or enteroclysis, can be
helpful
7/14/2025
56.
56
Cont…
For standardsmall bowel series,
contrast is swallowed or instilled into
the stomach through NGT
Abdominal radiographs are then taken
serially as the contrast travels distally in
the intestine
7/14/2025
57.
57
Cont…
Although bariumcan be used, water-soluble contrast
agents
Gastrograffin, should be used if the possibility of intestinal
perforation exists
These examinations are more labor-intensive and less
rapidly performed than CT scanning
But may offer greater sensitivity in the detection of
luminal and mural etiologies of obstruction, such as
primary intestinal tumors
7/14/2025
58.
58
Cont…
For enteroclysis,200-250 mL of barium followed
by 1-2 L of a solution of methylcellulose in water
is instilled into the proximal jejunum by NGT
The double contrast technique used in
enterocolysis permits
Better assessment of mucosal surface and
Detection of relatively small lesions, even through
overlapping small bowel loops
7/14/2025
59.
59
Cont…
Enterocolysis israrely performed in the acute
setting
But offers greater sensitivity than small bowel
series in the detection of lesions that may be
causing partial small bowel obstruction
Recently, CT enterocolysis has been used, and
It was reported to be superior to plain X-ray small
bowel contrast studies
7/14/2025
60.
60
Therapy
SBO isusually associated with a marked depletion of
intravascular volume due to
Decreased oral intake
Vomiting
Sequestration of fluid in bowel lumen and wall
Therefore, fluid resuscitation is integral to treatment
Isotonic fluid should be given intravenously, and
An indwelling bladder catheter may be placed to monitor
urine output
7/14/2025
61.
61
Cont…
Central venousorpulmonary-artery catheter
monitoring are not generally indicated
Unless the patient has underlying cardiac disease
and severe dehydration
Broad-spectrum antibiotics are not indicated
Unless there is concern for bowel ischemia and
surgery is planned
7/14/2025
62.
62
Cont…
The stomachshould be continuously
evacuated of air and fluid using NGT
Effective gastric decompression
decreases
Nausea
Distention
Risk of vomiting
Aspiration
7/14/2025
63.
63
Cont…
While aperiod of close observation and
nonoperative management has been the
mainstay of treatment for partial bowel
obstruction
The standard therapy for complete small
bowel obstruction has generally been
expeditious surgery
With the dictum that “the sun should never rise
and set on a complete bowel obstruction
7/14/2025
64.
64
Cont…
The rationalefor favoring early surgical
intervention is to minimize the risk for
bowel strangulation
Whichh is associated with an increased
risk for morbidity and mortality
7/14/2025
65.
65
Cont…
Obstruction priorto the onset of
irreversible ischemia
Therefore, the goal is to operate
before the onset of irreversible
ischemia
7/14/2025
66.
66
Cont…
This treatmentapproach has, however,
undergone significant reassessment in recent
years
Many advocating for nonoperative
approaches in management of these patients
After ruled out closed-loop obstruction is and
There is no evidence of intestinal ischemia
7/14/2025
67.
67
Cont…
Thus, conservativetherapy in the form
of NG decompression and fluid
resuscitation is now commonly
recommended
In the initial management of non ischemic
bowel obstruction
7/14/2025
68.
68
Cont…
Nonoperative managementhas been
documented to be successful in 65-81% of
patients with partial small bowel obstruction
Of those successfully treated nonoperatively
Only 5-15% have been reported to have
symptoms
That were not substantially improved within 48
hrs after initiation of therapy
7/14/2025
69.
69
Cont…
Therefore, mostpts with partial SBO whose
symptoms do not improve within 48 hrs after
initiation of non operative therapy should be
considered for surgery
The observation that administration of water-
soluble oral contrast has not only diagnostic
but also therapeutic and prognostic value
7/14/2025
72
Cont…
The operativeprocedure performed for small bowel
obstruction varies according to the etiology of the
obstruction
Adhesions are lysed
Tumors are resected
Hernias are reduced and repaired
Regardless of the etiology, the affected intestine should
be examined, and
Nonviable bowel should be resected
7/14/2025
73.
73
Cont…
Criteria suggestingviability are
Normal color
Peristalsis, and
Marginal arterial pulsations
Usually, visual inspection alone is adequate in judging
viability In borderline cases
A Doppler probe may be used to check for pulsatile flow to
the bowel, and
Arterial perfusion can be verified by visualizing
intravenously administered fluorescein dye in the bowel
wall under ultraviolet illumination
7/14/2025
74.
74
Cont…
In general,if the patient is
hemodynamically stable, short lengths
of bowel of questionable viability
Should be resected, and
Primary anastomosis of the remaining
intestine should be performed
7/14/2025
75.
75
Cont…
However, ifthe viability of a large proportion of
the intestine is in question, a concerted effort to
preserve intestinal tissue should be made
In such situations, the bowel of uncertain
viability should be left intact and
The patient reexplored in 24-48 hours in a
“second-look” operation
At that time, definitive resection of nonviable
bowel is completed
7/14/2025
76.
76
Cont…
Successful laparoscopicsurgery for bowel
obstruction is being reported with greater frequency
In a propensity score matched study of patients
Who underwent adhesiolysis for small bowel
obstruction
The laparoscopic approach was associated with
significantly lower rates of overall complications
Surgical site infections
A shorter length of hospital stay (4 vs. 10 days)
7/14/2025
77.
77
Cont…
Since distendedloops of bowel can interfere with
adequate visualization, early cases of proximal
small bowel obstruction
That are likely due to a single adhesive band are
best suited for this approach
Presence of bowel distention and multiple
adhesions can cause these procedures to be
difficult, with a reported conversion rate of 17-33%
7/14/2025
78.
78
Cont…
One ofthe major concerns with the
laparoscopic approach has been the risk
of iatrogenic bowel injury
Although the laparoscopic approach
was associated with greater surgical
time
7/14/2025
79.
79
Outcomes
The perioperativemortality rate associated
with surgery for non strangulating small
bowel obstruction is less than 5%
With most deaths occurring in elderly
patients with significant comorbidities
Mortality rates associated with surgery
for strangulated obstruction is higher
7/14/2025
80.
80
Cont…
Long-term prognosisis related to the etiology
of obstruction
Many patients who are treated
conservatively for adhesive small bowel
obstruction do not require future
readmissions
Less than 20% of such patients will have a
readmission over the subsequent 5 years with
another episode of bowel obstruction
7/14/2025
82
Introduction
Adhesive smallbowel obstruction is one of
the leading causes of surgical emergencies
and
In particular of surgical emergencies that
require an emergent operations
In the UK, SBO was the indication for 51%
of all emergency laparotomies
7/14/2025
83.
83
Cont…
Seven emergencysurgical procedures that account
for 80% of all general surgery emergency
admissions, morbidity, deaths, and healthcare
expenditures in the USA
Adhesive small bowel obstruction was the most
common diagnosis for both the top 2 (small bowel
resection) and top 5 (adhesiolysis) procedures
Operative adhesions are the leading cause of small
bowel obstructions, accounting for 60% of cases
7/14/2025
84.
84
Cont…
ASBO causesconsiderable harm
Resulting in 8 days of hospitalization on
average and
Hospital mortality rate of 3% per episode
Between 20 and 30% of patients with
ASBO require operative treatment
7/14/2025
85.
85
Cont…
Length ofhospitalization and
morbidity depend on the need for
surgical intervention
Average hospitalization after
surgical treatment of ASBO is 16 days
5 days following non-operative treatment
7/14/2025
86.
86
Peritoneal adhesions
Adhesionsis fibrous tissue that connects
surfaces or organs within the peritoneal
cavity that are normally separated
Such adhesions are the results of a
pathological healing response of the
peritoneum up on injury
As opposed to the normal “ad integrum” repair
7/14/2025
87.
87
Cont…
Typical adhesionsform after peritoneal injury
from abdominal surgery
Other conditions that may cause peritoneal injury
resulting in adhesion formation include
Radiotherapy
Endometriosis
Inflammation
Local response to tumors
7/14/2025
88.
88
Cont…
Adhesions froma non-operative etiology are
often part of a more complex pathology
That can cause chronic pain and complications
as the result of adhesions and other
mechanisms
Management of chronic abdominal
complications by adhesiolysis is controversial
7/14/2025
89.
89
Adhesive small bowelobstruction
Adhesions are the single most common
cause for small bowel obstruction
Definitive confirmation of the adhesive
etiology of bowel obstruction is made
during operative treatment
7/14/2025
90.
90
Cont…
Methods toconfirm the adhesive etiology of
bowel obstruction non invasively include
History of previous episodes of bowel obstruction
by adhesions or
Exclusion of other causes of bowel obstruction by
imaging (often CT scan)
7/14/2025
91.
91
Adhesiolysis
Adhesiolysis refersto releasing adhesions
either by blunt or sharp dissection during
surgery
It can be the primary indication for an
operation, as in a reoperation for small bowel
obstruction caused by adhesions
7/14/2025
92.
92
Cont…
Adhesiolysis isalso performed during reoperations
for indications no related to adhesions in order to
obtain sufficient access to the operative field
Complicated adhesiolysis refers to the event of
inadvertent injury while performing adhesiolysis
Injuries during adhesiolysis are most frequently
made to the bowel
7/14/2025
94
Epidemiology
The riskof SBO is highest following
Colorectal
Oncologic gynecological, or
Pediatric surgery
1 in 10 pts develops at least one episode of
SBO within 3 years after colectomy
7/14/2025
95.
95
Cont…
Reoperations forASBO occur in
Between 4.2 and 12.6% of pts after pediatric surgery pts
3.2% of colorectal pts
Recurrence of ASBO is also frequent
12% of non-operatively treated patients are readmitted within 1 year
Rising to 20% after 5 years
The risk of recurrence is slightly lower after operative
treatment:
8% after 1 year and
16% after 5 years
7/14/2025
96.
96
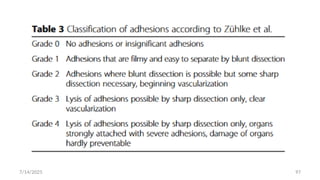
Classification of adhesions
The most frequently used classification of adhesions in
general surgery is the adhesion score according to Zühlke et al
The score is based on the
Tenacity and
Some morphologic aspects of the adhesions
The major drawback to the score is that it does not measure
the extent of adhesions and
Tenacity of adhesions can vary between different parts of the
abdomen
7/14/2025
98
Cont…
The mostused grading system in gynecological surgery is
the American Fertility Society (AFS) scor
The score is designed for grading adhesions in the small
pelvis
Adhesions are scored for extent and severity at four sites:
Right ovary
Right tube
Left ovary
Left tube
7/14/2025
99.
99
Cont…
The scoresfor the right and left side are summed, and the
final AFS score is the score for the side with the lowest
summed score while discarding the score for the other
side
Thus, a patient with an AFS score of 0 can still have
adhesions
Further critiques for this score include a relatively low
inter observer reproducibility
7/14/2025
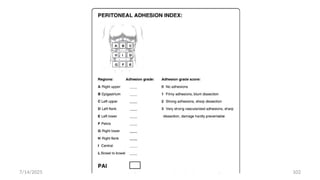
100.
100
Cont…
Recently introducedscore by the ASBO
working group is the peritoneal adhesion
index (PAI)
Which measures tenacity on a 1–3 scale at 10
predefined sites, to integrate tenacity and
extent of adhesions in a single score
7/14/2025
101.
101
Cont…
This scoreis the only score that has been
validated to be prognostic for convalescence
after surgery for ASBO and
The risk of injuries during adhesiolysis
7/14/2025
103
Prevention of adhesion
Surgicaltechnique
The main principles of prevention of adhesion and
related complications are
Minimizing surgical trauma and
Use of adjuvants to reduce adhesion formation
Laparoscopy is often believed to reduce adhesion
formation and the risk for ASBO
7/14/2025
104.
104
Cont…
Important riskfactors for aggravated
adhesion formation are worth considering
One of the most important risk factors is the
foreign body reaction
Starch-powdered gloves
Meshes used for abdominal wall reconstruction
7/14/2025
105.
105
Cont…
The choiceof energy device might also impact
adhesion formation
Peritoneal injury is
Lower in bipolar electrocautery and ultrasonic
device
Higher in monopolar electrocautery
7/14/2025
106.
106
Cont…
Animal data suggestthat both systemic and
intraperitoneal application of antibiotics, and
metronidazole in particular, can reduce adhesion
formation in septic conditions
7/14/2025
107.
107
Adhesion barriers
Adhesionbarriers are adjuvants for peritoneal
administration
That can effectively reduce adhesion formation.
Adhesion barriers are produced in several forms:
Solid membranes
Gels
Liquids
7/14/2025
108.
108
Cont…
The conceptbehind barriers is that they do not
actively interfere with inflammation and wound
healing
Rather, they act as a spacer
Which separates injured surfaces of the peritoneum,
Allowing these surfaces to heal without forming
fibrinous attachments which eventually lead to
adhesions
7/14/2025
111
Approach to thepatient with ASBO
The initial diagnosis of ASBO is of the most
importance
Failure to diagnose or having a delayed
diagnosis represents 70% of malpractice
claims in ASBO
7/14/2025
112.
112
Cont…
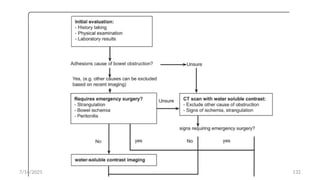
The primarygoals in the initial evaluation of
patients in whom adhesive small bowel
obstruction is suspected are
i. Differentiating between ASBO and other causes of
bowel obstruction
ii. Assessing the need for urgent surgical exploration
iii. Identifying and preventing complications from
bowel obstruction
7/14/2025
113.
113
History taking andphysical examination
ASBO is clinically diagnosed in a patient with
Intermittent colicky abdominal pain
Distention, and nausea(with or without vomiting),
With or without absence of stools
• Although diagnosis of small bowel obstruction is
fairly certain in a patient in whom all of these
symptoms are present
7/14/2025
114.
114
Cont…
In ptswith incomplete obstruction, watery
diarrhea may be present
The presence of watery diarrhea can cause an
episode of ASBO to be mistaken for gastro-enteritis
Stools might also be present in patients with a
relatively high obstruction who are admitted early
after onset of symptoms
7/14/2025
115.
115
Cont…
During P/E,signs of peritonitis that might
reveal strangulation or ischemia should be
evaluated
Differential considerations that can be
assessed during P/E include the presence of
any abdominal wall or groin hernias
7/14/2025
116.
116
Cont…
The evaluationof ASBO by history taking and
P/E has a low sensitivity for detecting bowel
strangulation and ischemia
Sensitivity of P/E for detection of
strangulation is only 48%, even in experienced
hands
7/14/2025
117.
117
Laboratory tests
Theminimum of laboratory tests include
Blood count
Lactate
Electrolytes
CRP, and BUN/creatinine
Laboratory values that might indicate peritonitis are
CRP > 75 and
White blood cell count > 10.000/mm3
Although sensitivity and specificity of these tests are relatively
low
7/14/2025
118.
118
Cont…
Electrolytes areoften disturbed in patients with
a bowel obstruction
In particular, low values of potassium are frequently
found and need to be corrected
BUN/creatinine needs to be assessed as patients
with ASBO are frequently dehydrated which
could result in AKI
7/14/2025
119.
119
Imaging studies
Plain X-rays
The value of plain X-rays complementary to P/E is
limited
In high-grade obstruction, a triad of multiple air-fluid
levels, distention of small bowel loops, and
Absence of gas in the colon are pathognomonic for SBO
but overall sensitivity and specificity of plain x-rays are
low ~70%
7/14/2025
120.
120
Cont…
A largevolume pneumo peritoneum 2 to
bowel perforation in ASBO can also be
detected on plain X-rays
Preferably by an erect chest X-ray Plain X-rays
However, do not detect the more early signs
of peritonitis or strangulation
7/14/2025
121.
121
Water-soluble contrast studies
If the contrast has not reached the colon on
an abdominal X-ray taken 24 h following
administration of the contrast
This is highly indicative of failure of non-
operative management
7/14/2025
122.
122
Cont…
CT scansCurrent helical CT scans not only
have good test characteristics for diagnosing
small bowel obstruction
but also have approximately 90% accuracy in
predicting strangulation and the need for
urgent surgery
7/14/2025
123.
123
Cont…
Diagnostic valueof CT scan can be enhanced
with the use of water-soluble contract
As with water-soluble contrast studies,
progress of the contrast can be evaluated by
X-ray at24 h after CT scan
7/14/2025
124.
124
Management
Initial decision making
Non-operative management should always be
tried in patients with ASBO
Unless there are signs of peritonitis, strangulation,
or bowel ischemia
7/14/2025
125.
125
Cont…
Although therisk of recurrence is slightly lower after
operative treatment
This is not a reason to opt for a primary surgical approach
Morbidity from emergency surgical exploration is high
There is a considerable risk for bowel injury, and
Surgical treatment may significantly reduce post-
operative quality of life
7/14/2025
126.
126
Non-operative management
Thecornerstone of non-operative
management is
Nil peros(NPO)
Decompression using a NGT or long intestinal tube
Non-operative management is effective in
approximately 70–90% of patients with ASBO
7/14/2025
127.
127
Cont…
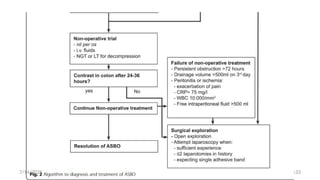
Continuing non-operativetreatment for more
than 72 h in cases with persistent high output
from a decompression tube,
But no other signs of clinical deterioration
however, remains subject to debate
7/14/2025
128.
128
Cont…
Common medicalcomplications in patients
with SBO are
Dehydration with kidney injury
Electrolyte disturbances
Malnutrition
Aspiration
7/14/2025
129.
129
Cont…
Non-operative management: summary
Evidence for the optimal duration of non-
operative is absent
But, most authors and the panel consider a
72-h period as safe and appropriate
7/14/2025
130.
130
Operative treatment
1) Laparatomy
2)Laparoscopy
The potential benefits of laparoscopy include
Less extensive adhesion (re)formation
Earlier return of bowel movements
Reduced post-operative pain, and
Shorter length of stay
7/14/2025
131.
131
Cont…
Operative management: summary
Laparoscopic surgery has been introduced in recent years
and might decrease morbidity in subgroups of patients
undergoing surgery for ASBO
The risk of bowel injuries seems higher in laparoscopic
surgery for ASBO
Therefore, careful selection of patients for laparoscopic
surgery is required
7/14/2025
134
Special patient groups
Youngpatients
The risk of adhesion-related complications is life-long
Although most small bowel obstructions will occur within
the first 2 years after surgery
New cases continue to develop many years after the
primary operation
Pediatric patients, who are at the extreme of young age,
have a high risk for adhesion-related complications
7/14/2025
135.
135
Young patientstherefore might have
the highest lifetime benefit from
adhesion prevention
No trials with adhesion barriers have
been performed in pediatric surgery
After a follow-up of 24 months, 2.0% of pediatric patients operated with adhesion
barrier versus 4.5% of patients operated on without adhesion barrier developed
ASBO
7/14/2025
136.
136
Elderly patients
Patientswith diabetes were shown to suffer
from a
7.5% incidence of AKI and
4.8% incidence of MI
If the incidence of these complications was
significantly higher when compared to diabetic
patients that were operated within 24 h and non-
diabetic patients with delayed operation
7/14/2025
137.
137
Pregnancy
SBO inpregnancy is very rare
But represents an important clinical
challenge with significant risk of fetal
loss
7/14/2025
140
Other Causes ofSBO
Early postoperative bowel obstruction
defined by signs, symptoms, and radiographic
signs of SBO
Occurring within 30 days following surgery
Maingoats 13th
ed says “6 weaks post operative”
been reported to occur in 0.7% to 9% of patients,
With a higher rate in patients undergoing pelvic
surgery, especially colorectal procedures
7/14/2025
141.
141
Cont…
CT scanningor small bowel series is often
required to make the diagnosis
Obstruction that occurs in the early
postoperative period is usually partial and
Only rarely is associated with
strangulation
7/14/2025
142.
142
Cont…
Therefore, aperiod of extended non
operative therapy (2–3 wks) consisting
of
Bowel rest
Hydration
TPN administration
7/14/2025
143.
143
However, expeditiousreoperation
should be undertaken without delay if
Complete obstruction is demonstrated
Signs suggestive of peritonitis are
detected
In a series of 180 patients undergoing anterior resection for rectal cancer,
12.8% developed early postoperative bowel obstruction on the median
postoperative day 5, with 4 requiring surgical exploration at a median interval
of 2 weeks from the index case
7/14/2025
144.
144
Cont…
Malignant small bowelobstruction
Although it often indicates advanced disease with
poor prognosis
25-33% of patients with a history of cancer
Who present with SBO have adhesions as the
etiology of their obstruction and
Therefore should not be denied appropriate
therapy
7/14/2025
145.
145
Even incases in which the obstruction is related to
recurrent malignancy
Palliative resection or bypass can be performed
In select cases these procedures lead to improved quality
of life
In a series of 81 patients with small bowel obstruction, palliation was achieved in
over 80% of patients, with over 70% able to reestablish oral intake. In this series,
the surgical morbidity was high, with 7% developing an enterocutaneous
fistula/anastomotic leak and a 30-day mortality rate of 6%
7/14/2025
146.
146
Cont…
Patients withobvious carcinomatosis and
multifocal obstruction pose a difficult challenge,
given their limited prognosis
At the time of surgery, relief of the obstruction
may be best achieved by
A bypass procedure
Avoiding a potentially difficult bowel resection
Even if that is not feasible, a palliative gastrostomy tube
can be considered to help resolve nausea and vomiting
7/14/2025
147.
147
ILEUS AND OTHERDISORDERS OF
INTESTINAL MOTILITY
Ileus and intestinal pseudo-obstruction
are clinical syndromes caused by
impaired intestinal motility and
Are characterized by symptoms and signs
of intestinal obstruction in the absence of
lesion-causing mechanical obstruction
7/14/2025
148.
148
Cont…
Ileus isa temporary motility disorder
That is reversed with time as the inciting
factor is corrected
Chronic intestinal pseudo-obstruction
Comprises a spectrum of specific disorders
associated with irreversible intestinal
dysmotility
7/14/2025
149.
149
Cont…
Ileus isa major cause of morbidity in
hospitalized patients
A degree of intestinal ileus is a normal
physiological response to abdominal
surgery
Which often resolves quickly without any
long-term sequela
7/14/2025
150.
150
Cont…
When postoperativeileus is prolonged,
it can cause significant morbidity and cost
Prolonged postoperative ileus is the
most frequently implicated cause of
Delayed discharge following abdominal
operations
7/14/2025
153
Cont…
Following mostabdominal operations
or injuries
The motility of the gastrointestinal tract
is transiently impaired
7/14/2025
154.
154
Cont…
Among theproposed mechanisms
responsible for this dysmotility are
Surgical stress-induced sympathetic reflexes
Inflammatory response mediator release, and
Anesthetic/analgesic side effects
Each of which can inhibit intestinal motility
7/14/2025
155.
155
Cont…
The returnof normal motility generally
follows a characteristic temporal sequence
Small intestinal motility returning to normal
within the first 24 hours after laparotomy
Gastric within by 48 hrs of after laparatomy
Colonic motility returning to normal by 2-5 ds
7/14/2025
156.
156
Cont…
Since smallbowel motility is returned before
colonic and gastric motility
Listening for bowel sounds is not a reliable
indicator that ileus has fully resolved
Functional evidence of coordinated
Gastrointestinal motility in the form of passing
flatus or bowel movement is a more useful
indicator
7/14/2025
157.
157
Cont…
Resolution ofileus may be delayed in
the presence of other factors capable of
inciting ileus
Such as the presence of intra-abdominal
abscesses or electrolyte abnormalities
7/14/2025
158.
158
Cont…
Chronic intestinalpseudo-obstruction
can be caused by a large number of
specific abnormalities affecting intestinal
Smooth muscle
The myenteric plexus
Extraintestinal nervous system
7/14/2025
160
Cont…
Visceral myopathiesconstitute a group
of diseases characterized by
Degeneration and fibrosis of the intestinal
muscularis propria
Visceral neuropathies encompass a
variety of degenerative disorders of the
myenteric and submucosal plexuses
7/14/2025
161.
161
Cont…
Both sporadicand familial forms of visceral
myopathies and neuropathies exist
Systemic disorders involving the smooth
muscle such as
Progressive systemic sclerosis
Progressive muscular dystrophy
Neurological diseases
Parkinson’s disease, can also be complicated by chronic
intestinal pseudo-obstruction
7/14/2025
162.
162
Cont…
Viral infectionsassociated with a cause
of intestinal pseudo-obstruction
Cytomegalovirus
Epstein-Barr virus
7/14/2025
163.
163
Clinical Presentation
Inabilityto tolerate liquids and solids by
mouth
Nausea
Lack of flatus or bowel movements
Vomiting and abdominal distension
may occur
7/14/2025
164.
164
Cont…
Although bowelsound characteristics
are not diagnostic
They are usually diminished or absent
Hyperactive bowel sounds that usually
accompany mechanical small bowel
obstruction
7/14/2025
165.
165
Diagnosis
Routine postoperativeileus should be
expected and requires no diagnostic
evaluation
Definition of prolonged postoperative
ileus has been varied
But generally diagnosed if ileus persists
beyond 5 days postoperatively
7/14/2025
166.
166
A recent globalsurvey synthesized the results of the data to
define
Postoperative ileus is “interval from surgery until
passage of flatus/stool AND tolerance of an oral diet,”
With prolonged postoperative ileus being defined as
“Two or more of nausea/vomiting
Inability to tolerate oral diet over 24 h,
Absence of flatus over 24 h,
Distension
Radiologic confirmation occurring on or after day 4
postoperatively without prior resolution of postoperative ileus
7/14/2025
167.
167
Cont…
Prolonged ileusis reported to occur in 10-
15% of patients undergoing intestinal surgery
Medication lists should be reviewed
Abdominal radiographs are often obtained
But the distinction between ileus and
mechanical obstruction may be difficult based
on this test alone
7/14/2025
168.
168
Cont…
In thepostoperative setting
CT scanning is the test of choice
As it can demonstrate the presence of an
intra-abdominal abscess or
Other evidence of peritoneal sepsis that
may be causing ileus and
Can exclude the presence of complete
mechanical obstruction
7/14/2025
169.
169
Cont…
The diagnosisof chronic pseudo-obstruction is
suggested by clinical features and
Confirmed by radiographic and manometric
studies
Diagnostic laparotomy or laparoscopy with full-
thickness biopsy of the small intestine
May be required to establish the specific underlying
cause in cases of suspected neural disorder
7/14/2025
170.
170
Therapy
The managementof ileus consists of
Limiting oral intake and
Correcting the underlying inciting factor
If vomiting or abdominal distention are
prominent
The stomach should be decompressed using a
NGT
7/14/2025
171.
171
Cont…
Fluid andelectrolytes should be
administered intravenously until ileus
resolves
If the duration of ileus is prolonged,
total parental nutrition (TPN) may be
required
7/14/2025
172.
172
Cont…
Given thefrequency of postoperative ileus
and its financial impact, many strategies
have been tested to reduce its duration
The administration of NSAID such as
ketorolac and concomitant reductions in
opioid dosing have been shown to reduce the
duration of ileus in most studies
7/14/2025
173.
173
Cont…
Similarly theuse of perioperative thoracic
epidural anesthesia/analgesia with regimens
containing local anesthetics combined with
limitation or elimination of systemically
administered opioids has been shown to reduce
duration of postoperative ileus
Although they have not reduced the overall
length of hospital stay
7/14/2025
174.
174
Cont…
limiting intra-and postoperative fluid
administration can also result in reduction of
postoperative ileus and shortened hospital stay
Early postoperative feeding after GI surgery is
generally well tolerated and can lead to
reduced postoperative ileus and a shorter
hospital stay
7/14/2025
177
Cont…
Administration ofalvimopan, a novel,
peripherally active mu-opioid receptor
antagonist with limited oral absorption
Has been shown to reduce duration of
Postoperative ileus
Hospital stay
Rate of readmissions in several prospective
7/14/2025
178.
178
Cont…
The therapyof patients with chronic intestinal
pseudo obstruction focuses on palliation of
symptoms as well as
Fluid
Electrolyte
Nutritional management
Surgery should be avoided if possible
7/14/2025
179.
179
Cont…
No standardtherapies are curative or
delay the natural history of any of the
specific disorders causing intestinal
pseudo-obstruction
Prokinetic agents, such as
metoclopromide and erythromycin, are
associated with poor efficacy
7/14/2025
180.
180
Cont…
Patients withrefractory disease may require
strict limitation of oral intake and long-term TPN
administration
Despite these measures, some patients will
continue to have severe abdominal pain or
such copious intestinal secretions that vomiting
and fluid and electrolyte losses remain substantial
7/14/2025
181.
181
Cont…
These patientsmay require a decompressive
gastrostomy or an extended small bowel
resection to remove abnormal intestine
Small-intestinal transplantation has been applied
in these patients with increasing frequency;
The ultimate role of this modality remains to be
defined
7/14/2025
182.
182
Reference
Schwartzs principleof Surgery 11th
ed 2019
Shackel ford 8th
ed 2019
Bologna guidline 2018
7/14/2025
T
H
A
N
K
Y
O
U
!
!
!
Editor's Notes
#64 Clinical signs and currently available laboratory tests and imaging studies do not reliably permit the distinction between patients with simple obstruction and those with strangulated
#65 In a study of 145 patients with CT-diagnosed high-grade compete small bowel obstruction, 46% of the overall cohort were managed nonoperatively. More
specifically, of the 104 patients who did not meet criteria for immediate surgery, 66 patients were successfully managed nonoperatively
#71 Several studies and subsequent meta-analyses have shown that use of water-soluble contrast not only predicts likelihood of success of nonoperative
management but also reduces the need for surgery (odds ratio 0.44), length of stay by about 2 days, and time to resolution by about 28 hours, without an increase in morbidity or mortality
#73 Neither technique has, however, been found to be superior to clinical judgment
#103 In a systematic review of co-
hort studies, the incidence of reoperation for ASBO was
1.4 (95% CI 1.0–1.8%) after laparoscopic and 3.8% (95%
CI 3.1–4.4%) after open surgery
#123 Although adhesions are not directly visible even on CT
scan, a CT scan can differentiate accurately between dif-
ferent causes of bowel obstruction by excluding other
causes
#180 Cisapride has been associated with palliation of symptoms;
however, because of cardiac toxicity and reported deaths, this
agent is restricted to compassionate use in the United States



























































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)
