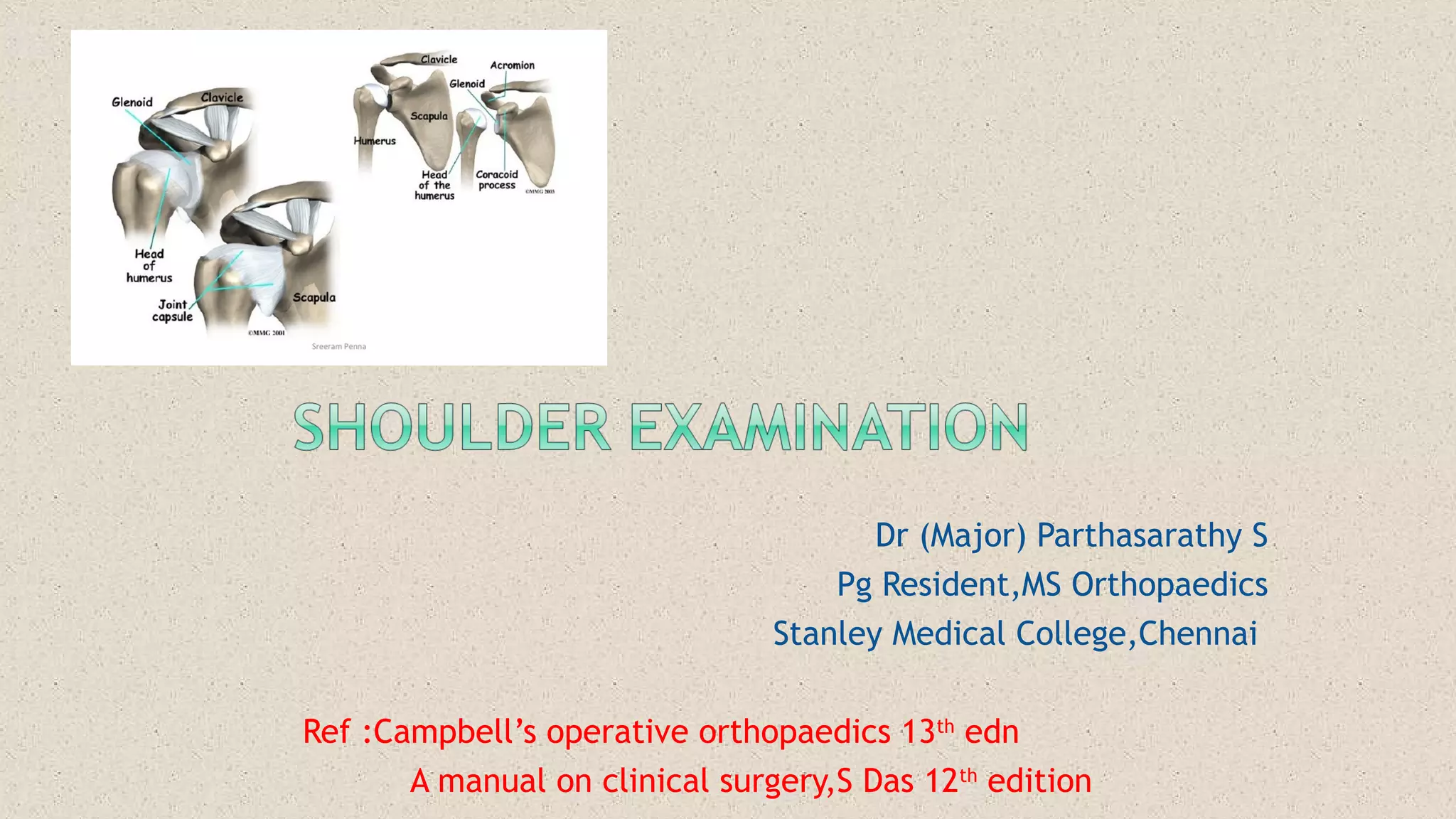
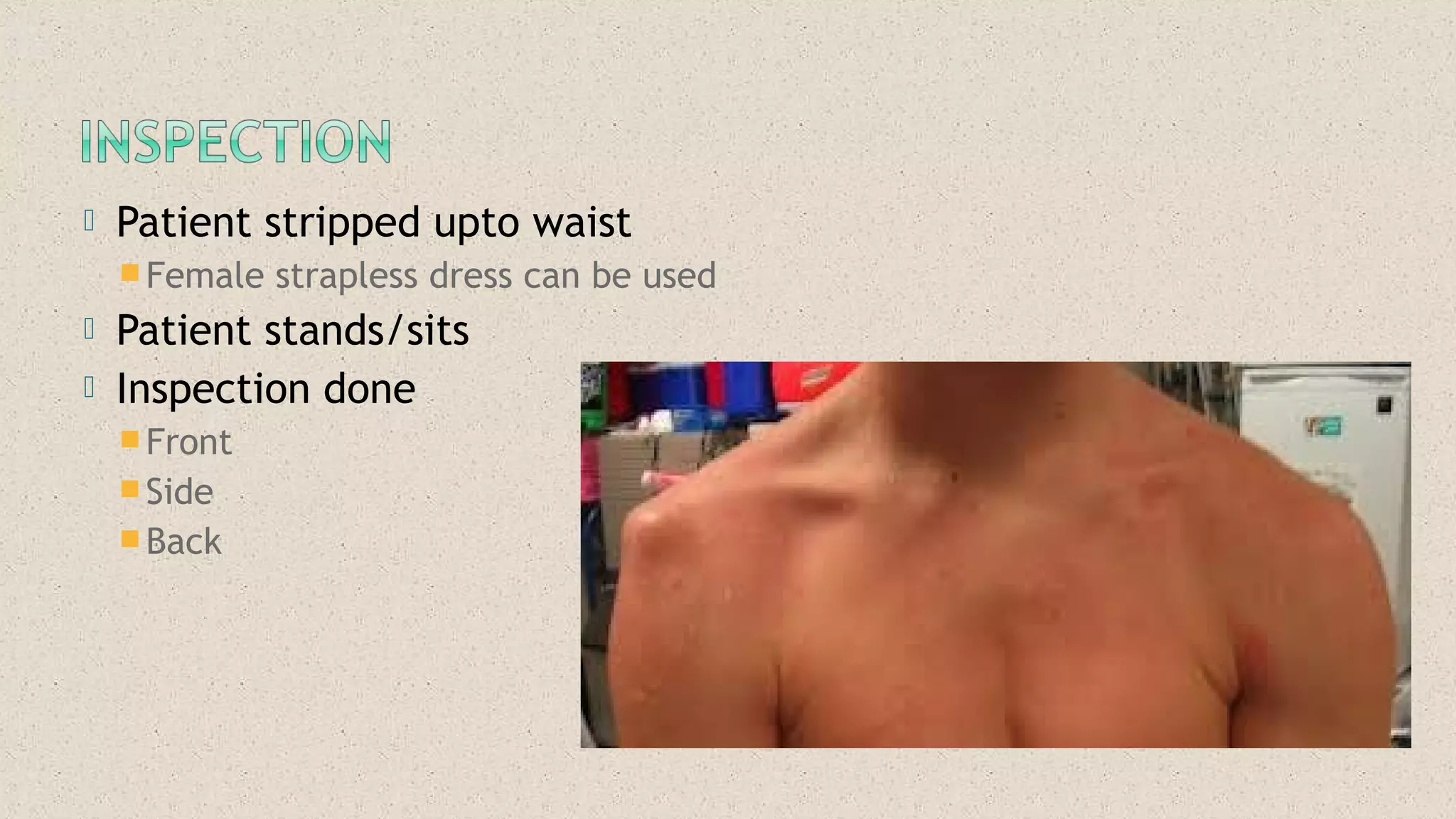
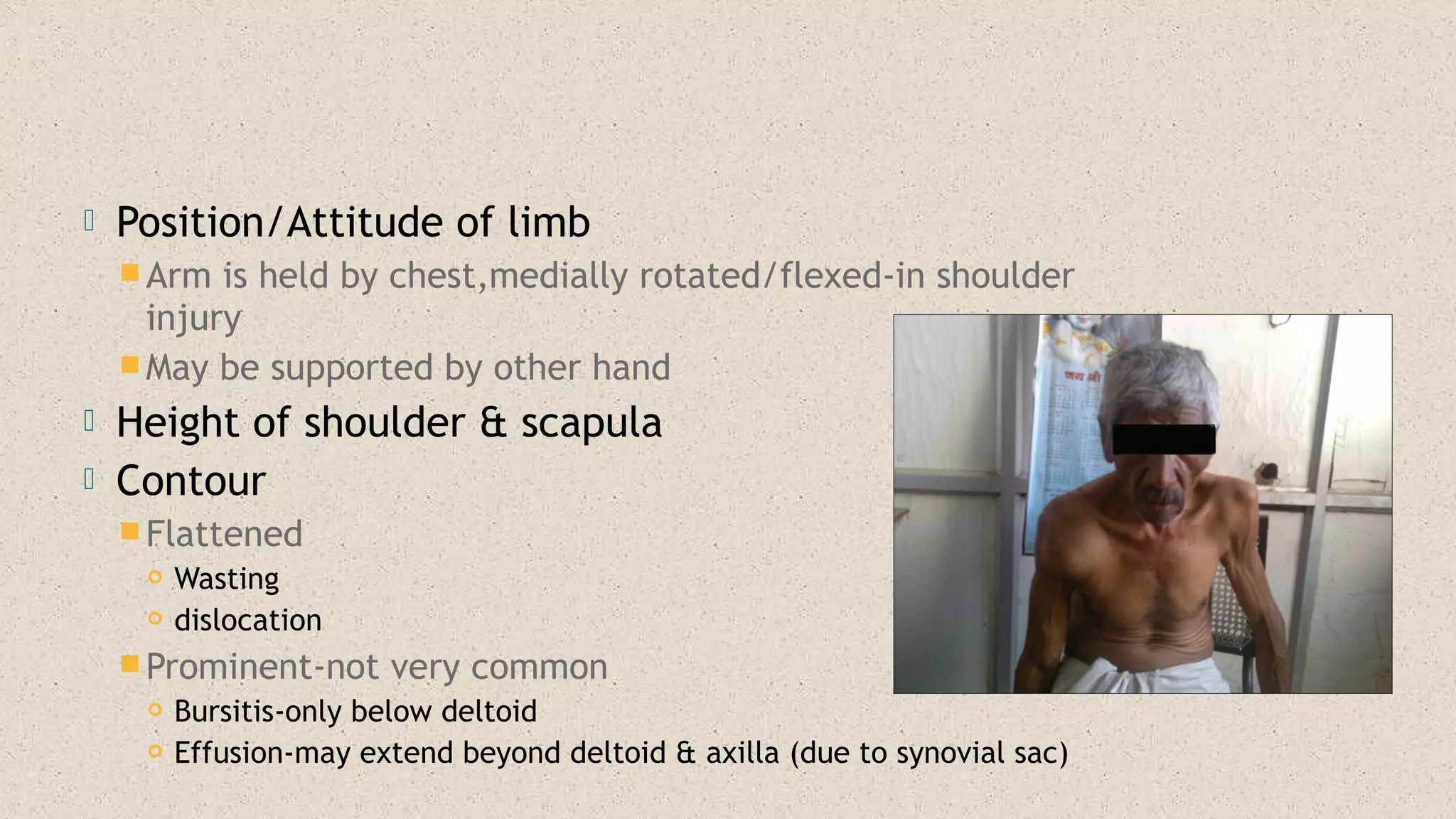
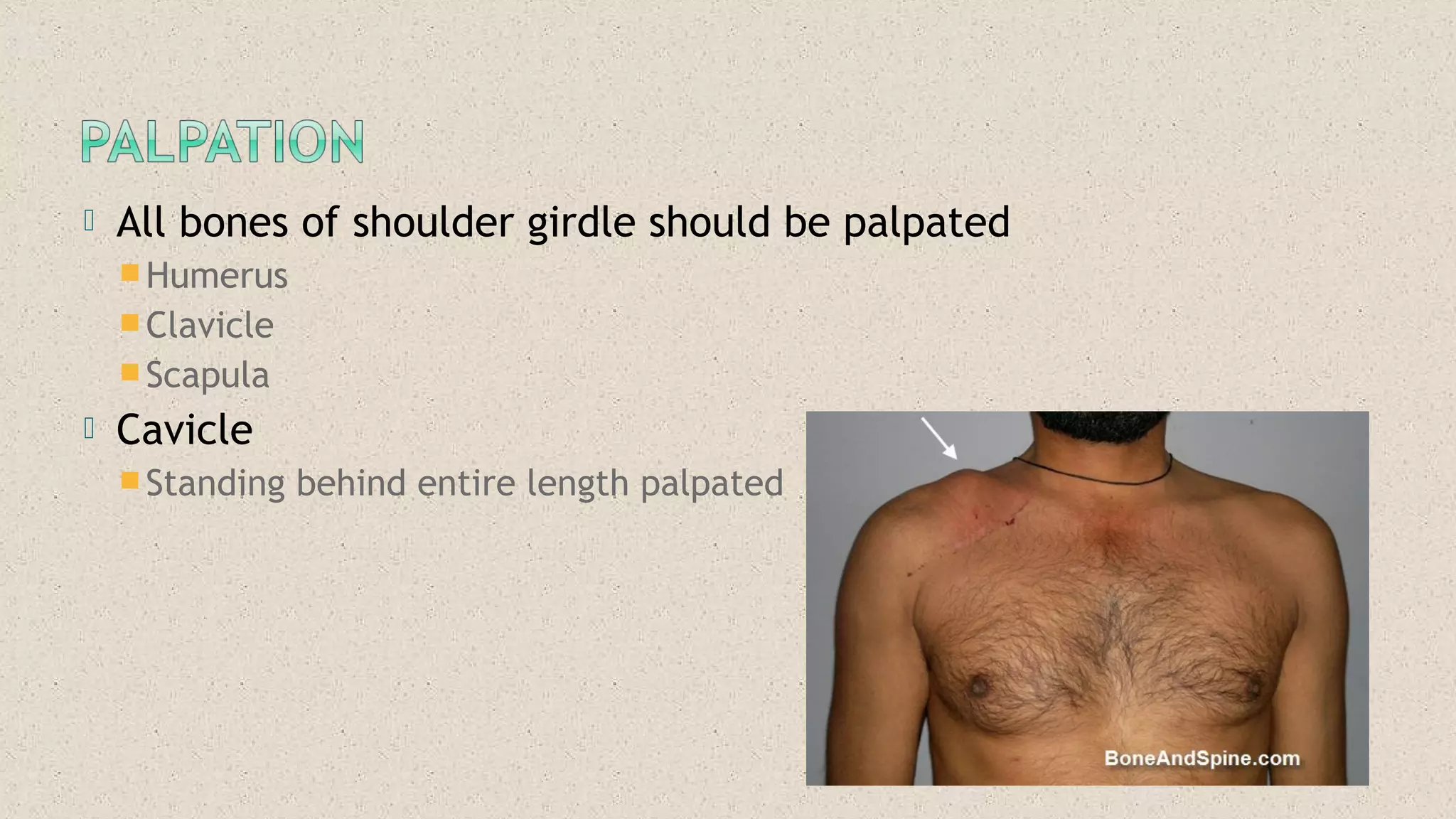
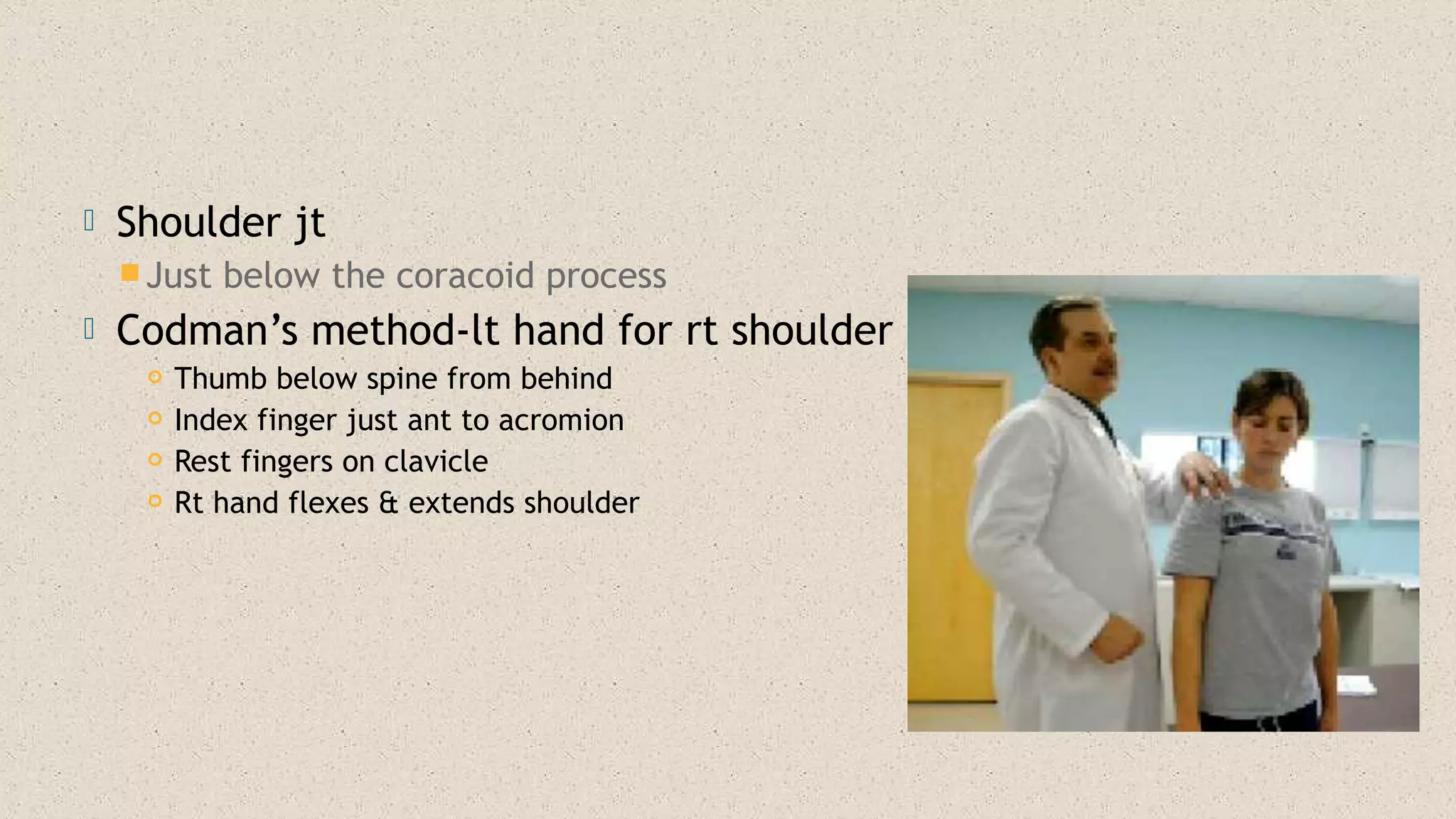
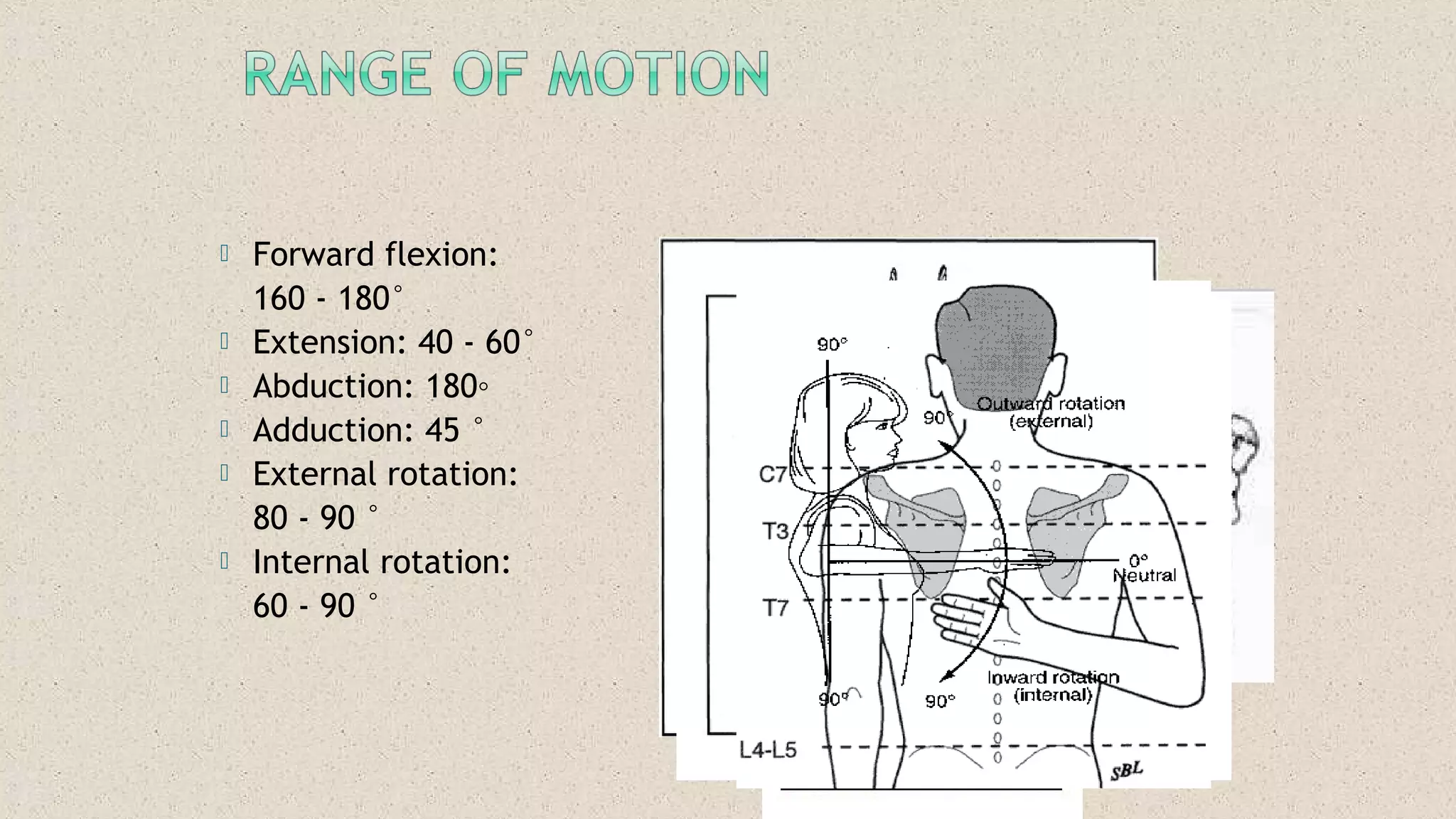
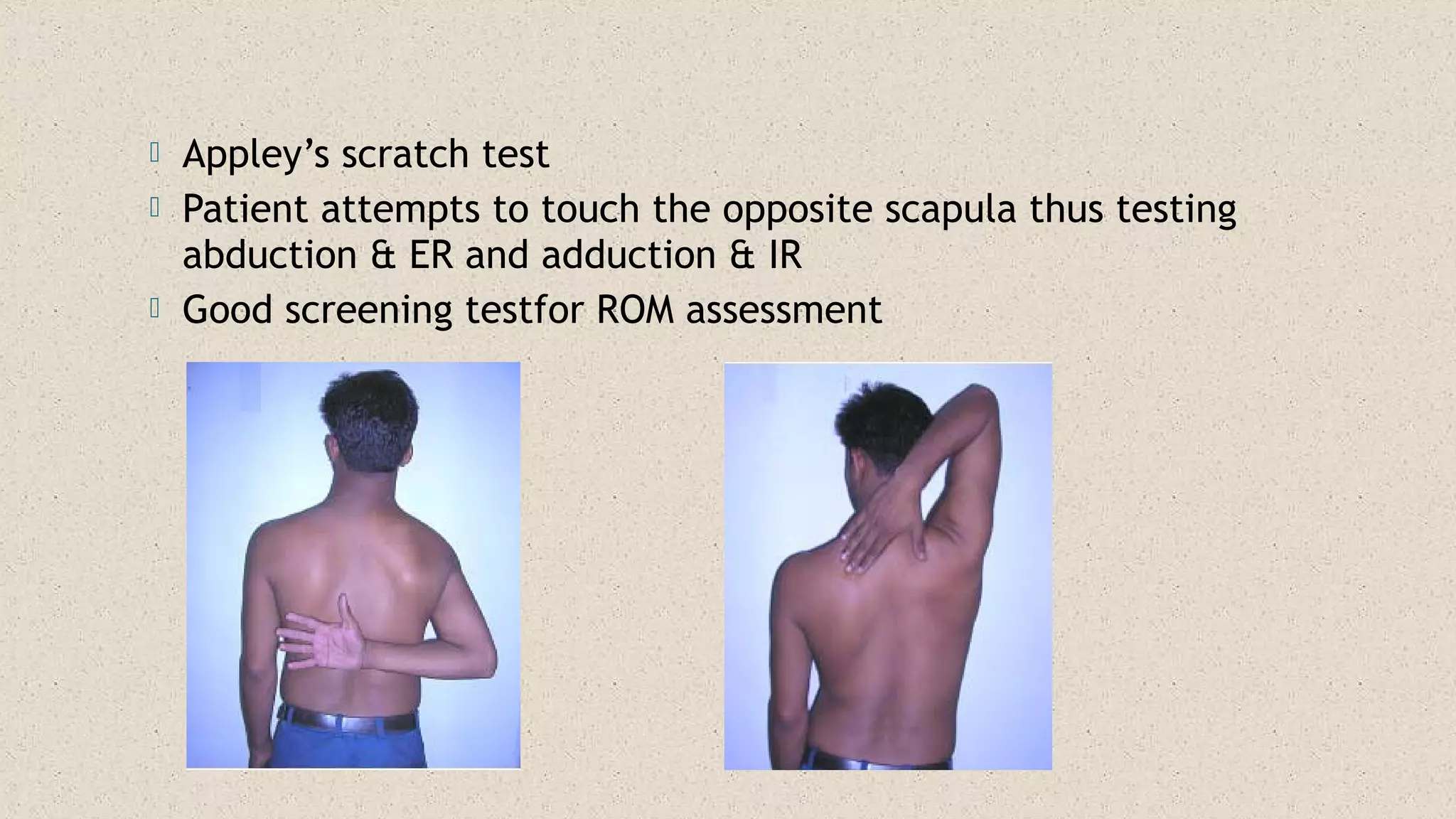
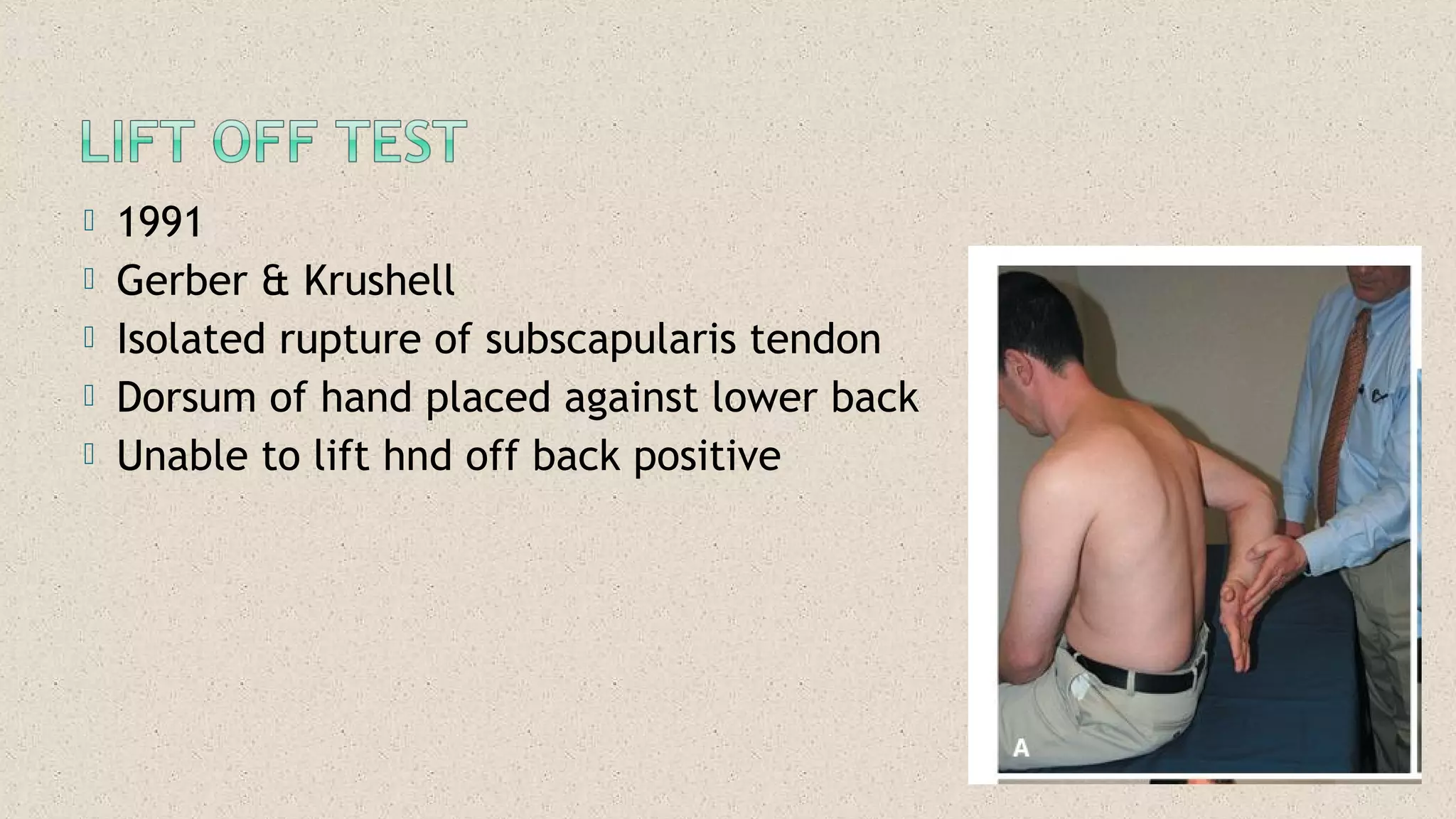
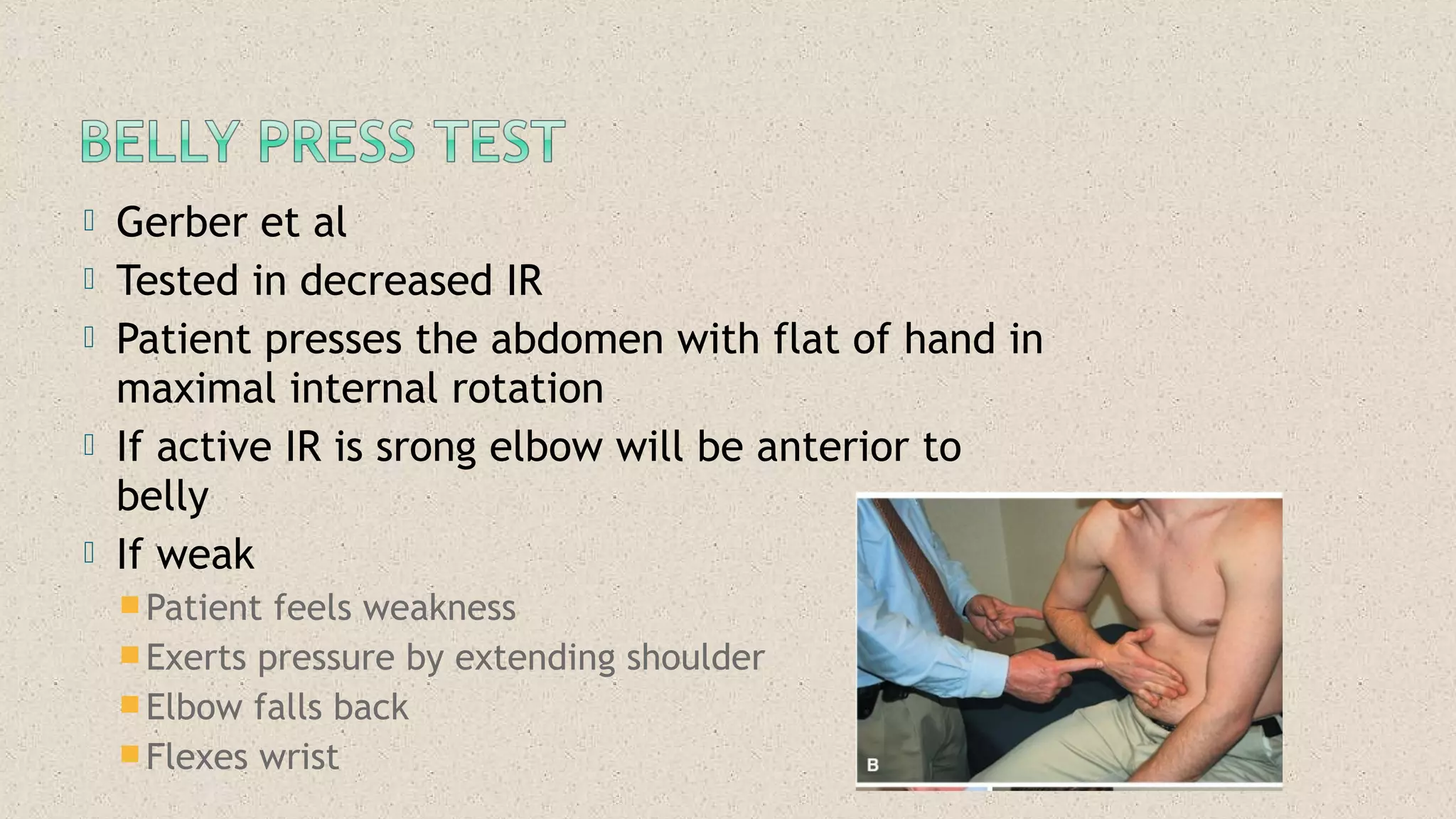
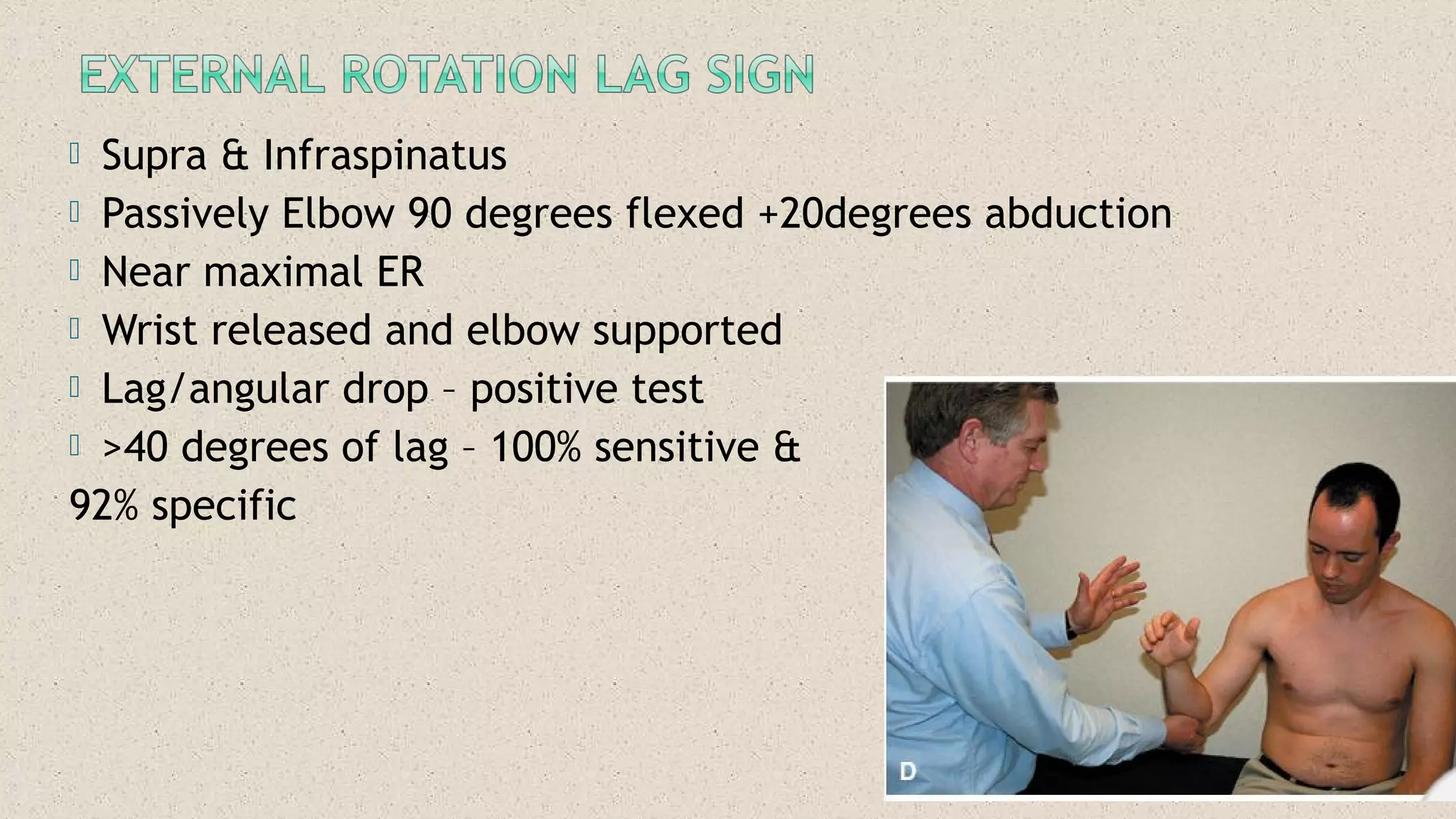
This document provides guidance on performing a physical examination of the shoulder, including inspection, palpation, range of motion testing, special tests, and measurements. Key steps outlined include inspecting the shoulder from multiple angles, palpating various bony landmarks and soft tissues, assessing range of motion in different planes, and performing special tests to evaluate for conditions like impingement, rotator cuff tears, labral tears, and instability. Detailed procedures are described for special tests to isolate involvement of specific shoulder structures.





















































































![Shoulder_joint_and_applied_aspects[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/shoulderjointandappliedaspects1-240425164911-e75cbd49-thumbnail.jpg?width=640&height=640&fit=bounds)






























