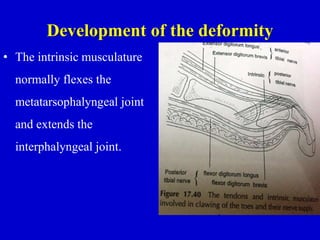
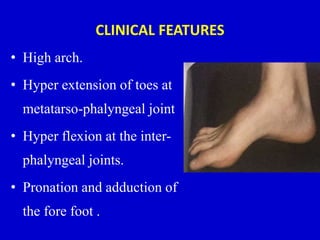
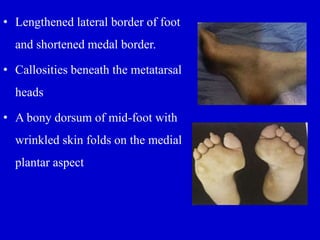
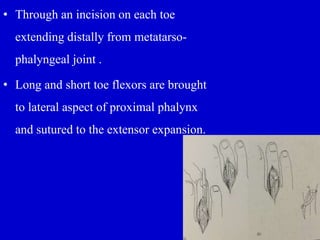
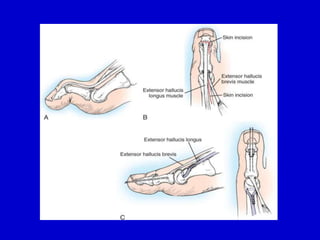
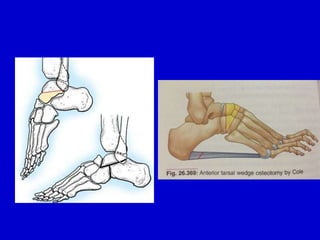
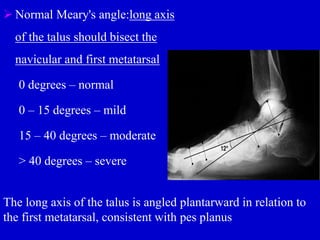
Pes cavus and pes planus are foot deformities characterized by high and low arches, respectively. Pes cavus, or a high arched foot, can be congenital or acquired and results in clawing of the toes. Pes planus, or a flat foot, is caused by the collapse of the medial longitudinal arch. Both conditions can cause foot, ankle, and leg pain and abnormal shoe wear. Treatment involves orthotics, physical therapy, and sometimes surgery to correct muscle imbalances and bony deformities.