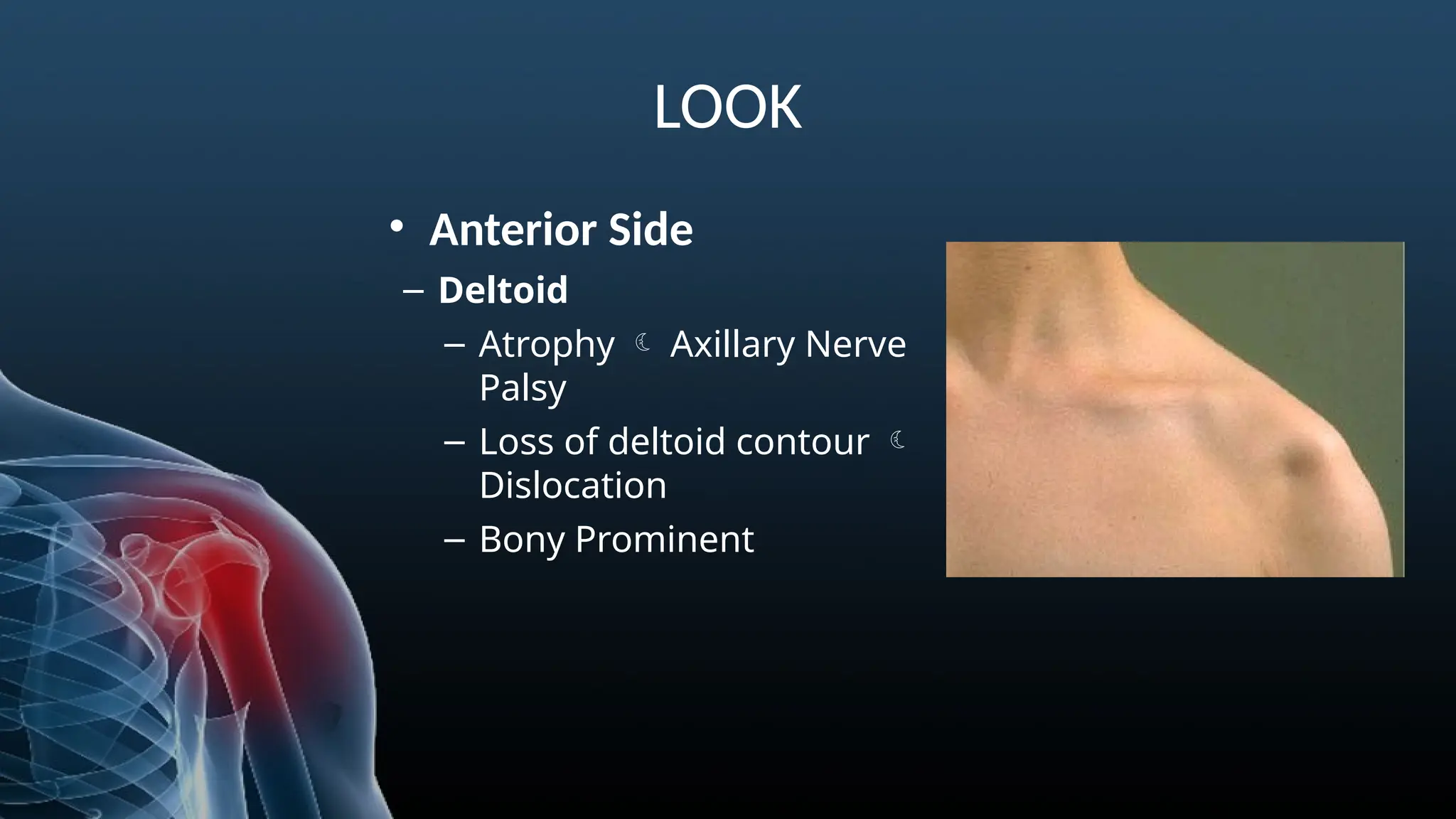
LOOK
•Borders of scapula
–lateral;prominent in
Latisimus dorsi atrophy
– superior; prominent
in supraspinatus &
trapezius atrophy
– Vertebral; prominent
in serratus ant
weakness/winging
SULCUS TEST
Detect inferiorinstability of the gleno-
humeral joint
“+” if dimpling of the skin below the
acromion or widening of the subacromial
space on palpation; >2cm translation
16.
Anterior and PosteriorDrawer
• Detect anterior and posterior instability
of the gleno-humeral joint
• Observe any movement, clicks and
patient apprehension.
• + if pain or apprehension by the client to
assume this position for fear of shoulder
dislocation
17.
APPREHENSION TEST
• Detectinstability of the gleno-humeral
joint
• Shoulder abducted to 90°, Slight stress to
humeral head directed in anterior
direction while externally rotating
shoulder
• + if pain or apprehension by the client to
assume this position for fear of shoulder
dislocation
18.
RELOCATION TEST
• DetectAnterior instability
• After a positive apprehension Apply
posteriorly directed force over
externally rotated humeral head
• Positive test is relief of
apprehension
NEER’S TEST
• Testfor impingement
• Passively take UE into full shoulder flexion
with humerus in Internal Rotation
• “+” if Pain located to the subacromial space
or anterior edge of acromion
• pain may be indicative of impingement of the
supraspinatus or long head of the biceps
21.
HAWKINS/KENNEDY TEST
• Testfor impingement
• place shoulder in 90° of flexion, slight
horizontal adduction, & maximal IR
• “+” if Pain located to the subacromial
space or anterior edge of acromion
• + test = shoulder pain due to
impingement of supraspinatus
between greater tuberosity against
coracoacromial arch
22.
JOBES TEST
• Testsupraspinatus muscle
• Elevate Upper Extrimity 30°–45° in
plane of the scapula with Internal
Rotation, resist elevation
• + test = reproduction of pain &/or
• weakness
23.
ROTATOR CUFF
• Externalrotation lag sign (ERLS)
• Hornblowers sign
• Internal rotation lag sign (IRLS)
• Belly Press Test
• Bear Hug Test
24.
External Rotation LagSign (ERLS)
• Test for infraspinatus tear.
• The clinician grasps the patient’s wrist and then
places the elbow at 90 degrees of flexion and the
shoulder at 20 degrees of elevation in the scapular
plane. Passively externally rotates the shoulder and,
at the end range, asks the patient to maintain this
position as the patient’s wrist is released
• A positive test, which is indicated by lag that occurs
with the inability of the patient to maintain his or her
arm near full External Rotation
25.
HORNBLOWERS SIGN
• Testteres minor muscle
• Shoulder in 90° abd & elbow flexed so that the
hand comes to the mouth (blowing a horn)
• + test = reproduction of pain &/or inability to
maintain Upper Extrimity in External Rotation
26.
Internal Rotation LagSign (IRLS)
• Test for Subscapularis tear
• clinician grasps the patient’s shoulder with one
hand and the wrist with the other and then lifts
the patient’s arm off the back. The clinician then
asks the patient to maintain this position as the
wrist is released.
• A positive test, which is manifested with an
inability of the patient to maintain his or her arm
off of the back
27.
BELLY PRESS TEST
•Test subscapularis muscle
• Press the hand into belly
• A positive test, which results in the elbow
dropping behind the body into extension,
indicates a subscapularis tear
28.
BEAR HUG TEST
•Test subscapularis tear
• The patient place the hand of the involved arm on the
contralateral acromioclavicular joint with the hand flat
and fingers extended. The elbow of the involved arm
should be positioned anterior to the body at the same
height as the shoulders. The patient is asked to maintain
that position while the examiner applies an ER force to
the forear
• A positive test is weakness or inability to maintain that
position
SPEED’S TEST
• Assessfor biceps tendonitis or labrum
problem
• Resist elevation
• + test = pain with biceps tendonitis & sense of
instability with labral px
31.
YERGASON’S TEST
• Assessfor Bisceps Tendon
• The patient sits or stands, and the upper arm
is positioned with the elbow at 90 degrees of
flexion and the forearm pronated. The patient
is asked to supinate his or her forearm against
the manual resistance of the clinician.
• + test = pain over the bicipital groove
32.
SLAP (Superior LabrumAnterior to Posterior)
Lession
• O’Briens Test
• Pain Provocation test
• Crank Test
• Jerk Test
• Kim Test
33.
O’BRIENS TEST
• AssessAssess for labrum or AC joint problem
• Resist elevation in Internal Rotation then
repeat in External Rotation
• + test = pain in IR > ER; pain “inside” shoulder
is labrum & pain “on top” of shoulder is AC
34.
PAIN PROVOCATION TEST
•Assess Assess for labrum
• Traction the biceps by passively taking the forearm
into maximal pronation
• + test = biceps will tug on labrum & reproduces the
pain in the superior region of the joint line (superior
labrum)
35.
CRANK TEST
• AssessAssess for labrum
• Their arm is elevated to 160 degrees in the scapular
plane of the body and is positioned in maximal
internal or ER. The clinician then applies an axial load
along the humerus.
• A positive test is indicated by the reproduction of a
painful click in the shoulder during the maneuver.
36.
JERK TEST
• Detecta posteroinferior labral lesion
• The clinician grasps the patient’s elbow with one
hand and the scapula with the other, and then
positions the patient’s arm at 90 degrees of
abduction and IR. The clinician then provides an axial
compression-based load to the humerus through the
elbow while maintaining the horizontally abducted
arm.
• A positive test is indicated by sharp shoulder pain
with or without a clunk or click
37.
KIM TEST
• Detecta posteroinferior labral lesion
• The clinician grasps the elbow with one hand and the
midhumeral region with the other hand, and then
elevates the patient’s arm to 90 degrees of
abduction. Simultaneously, the clinician provides an
axial load to the humerus and a 45-degree diagonal
elevation to the distal humerus concurrent with a
posteroinferior glide to the proximal humerus.
• A positive test is indicated by a sudden onset of
posterior shoulder pain.
38.
AC JOINT
• AcShear Test
• Coracoclavicular Ligament Test
• Cross-body Adduction Test
39.
AC SHEAR TEST
•Assess for AC sprain
• Clinician interlaces fingers & surrounds the AC joint;
squeezing the hands together compresses the AC
joint
• + test = pain or excessive move is indicative of
damage to the AC ligaments
40.
CORACOCLAVICULAR LIGAMENT TEST
•Assess CC ligament
• Place affected Upper Extrimity behind back, palpate
CC ligament while stabilizing clavicle; pulling inferior
angle of scapula away from ribs to stress the conoid
portion; pulling medial border of scapula away from
the ribs stresses the trapezoid portion
• + test = pain
• The anteriorsurgical approach offers good wide
exposure of the shoulder joint, allowing repairs to be
made of its anterior, inferior, and superior coverings.
• anterior approach permits the following :
– Reconstruction of recurrent dislocations
– Drainage of sepsis
– Biopsy and excision of tumors
– Repair or stabilization of the tendon of the long head of the biceps
– Shoulder arthroplasties, which usually are inserted through modified
anterior incisions
– Fixation of fractures of the proximal humerus
Anterior Approach
LANDMARKS AND INCISION
TwoSkin Incision:
• Anterior Incision
• Axillary Incision
Anterior Incision AxiIlary incision Retract the axillary incision cephalad
to expose the cephalic vein and the
deltopectoral groove.
46.
Superficial Surgical Dissection
Findthe deltopectoral groove, with its cephalic vein.
Retract the pectoralis major medially and the deltoid laterally,
splitting the two muscles apart
DANGER
Nerves
• musculocutaneous nerve
–Enters the body of the coracobrachialis to
the muscle's origin at the coracoid process.
– nerve enters the muscle from its medial
side, all dissection must remain on the
lateral side
– Do not to retract the muscle inferiorly, to
avoid stretching the nerve and causing
paralysis of the elbow flexors
Vessel
• cephalic vein
– The cephalic vein should be preserved
– traumatized cephalic vein should be ligated
to prevent the slight danger of
thromboembolism
50.
Lateral Approach
• Thelateral approach provides limited access to
the head and surgical neck of the humerus.
• The uses of the lateral approach include the
following:
– Open reduction and internal fixation of displaced fractures of
the greater tuberosity of the humerus
– Open reduction and internal fixation of humeral neck fractures
– Removal of calcific deposits from the subacromial bursa
– Repair of the supraspinatus tendon
– Repair of the rotator cuff
51.
POSITIONING
Position of thepatient on the operating table for the
lateral approach to the shoulder. Elevate the table 45°.
Place a
SANDBAG
52.
LANDMARK AND INCISION
LANDMARK
Theacromion is rectangular. Its bony dorsum and lateral border
are easy to palpate on the outer aspect of the shoulder.
INCISION
Make a 5-cm longitudinal incision from the tip of the acromion
down the lateral aspect of the arm
53.
• Superficial SurgicalDissection
Split the deltoid muscle in the line of its fibers from the
acromion downward for 5 cm. Insert a suture at the
inferior apex of the split to help prevent it from
extending accidentally, with consequent axillary nerve
damage, as the exposure is worked on
DANGER
Nerves
• The axillarynerve leaves the posterior
wall of the axilla by penetrating the
quadrangular space. Then it winds
around the humerus with the posterior
circumflex humeral arteries
56.
Posterior Approach
• Theposterior approach offers access to the posterior and
inferior aspects of the shoulder joinIt rarely is needed, but
can be used in the following instances :
– Repairs in cases of recurrent posterior dislocation or subluxation of the shoulder
– Glenoid osteotomy
– Biopsy and excision of tumors
– Removal of loose bodies in the posterior recess of the shoulder
– Drainage of sepsis (the approach allows dependent drainage with the patient in the normal
position in bed)
– Treatment of fractures of the scapula neck, particularly those in association with fractured
clavicles (floating shoulder)
– Treatment of posterior fracture dislocations of the proximal humerus
57.
POSITIONING
Place the patientin a lateral position on the edge of
the operating table with the affected side uppermost.
Drape him or her to allow independent movement of
the arm. Stand behind the patient and take care that
the ear is not folded accidentally under the head
58.
LANDMARK AND INCISION
Landmarks
Theacromion and the spine of the scapula form one
continuous arch. The spine of the scapula extends
obliquely across the upper four fifths of the dorsum of
the scapula and ends in a flat, smooth triangle at the
medial border of the scapula. It is easy to palpate.
Incision
Make a linear incision along the entire length of the
scapular spine, extending to the posterior corner of the
acromion
61.
DANGER
Nerves
• The axillarynerve runs through the
quadrangular space beneath the teres
minor.
• The suprascapular nerve passes
around the base of the spine of the
scapula as it runs from the
supraspinous fossa to the infraspinous
fossa.
Vessel
• The posterior circumflex humeral
artery runs with the axillary nerve in
the quadrangular space beneath the
inferior border of the teres minor
muscle. Damage to this artery leads to
hemorrhaging that is difficult to
control. This danger can be avoided by
staying in the correct intermuscular
plane
#47 1. Retract the pectoralis major medially and the deltoid laterally to expose the conjoined tendon of the short head of
the biceps and coracobrachialis muscle. Drill the tip of the coracoid process before cutting it. Incise the fascia on the lateral
aspect of the conjoint tendon. Note the leash of vessels at the inferior end of the subscapularis muscle
2. Cut through the predrilled coracoid process. Retract the conjoint tendon medially to give greater exposure to the
subscapularis tendon.
#48 1. Insert a curved artery clamp under the subscapularis muscle. A leash of vessels at the caudal end of the wound marks
the lower border of the subscapularis.
2. Incise the end of the subscapularis. Tag and place stay sutures into the muscle to prevent it from retracting medially.
Some of the subscapularis fibers insert directly into the joint capsule.
3. Incise the joint capsule longitudinally to expose the humeral head and the glenoid cavity.
#54 Expose the subdeltoid portion of the subacromial bursa by retracting the deltoid muscle anteriorly and posteriorly
Incise the bursa to reveal the insertion of the supraspinatus tendon into the greater tuberosity.
























































































![Shoulder_joint_and_applied_aspects[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/shoulderjointandappliedaspects1-240425164911-e75cbd49-thumbnail.jpg?width=640&height=640&fit=bounds)







































