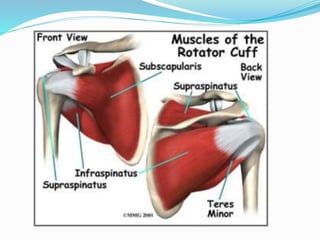
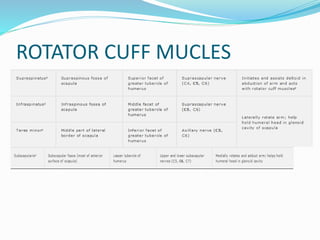
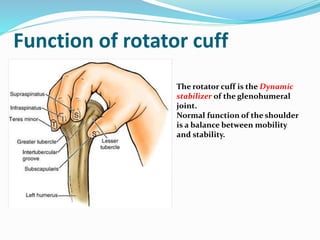
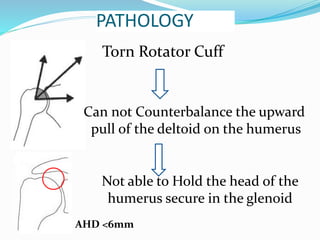
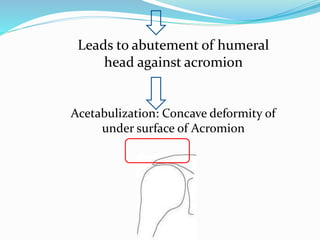
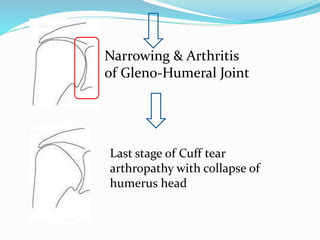
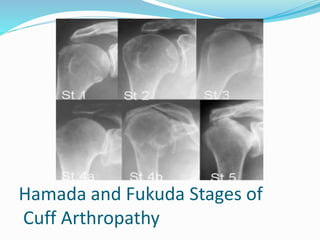
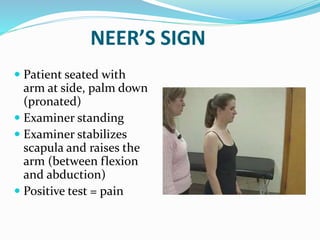
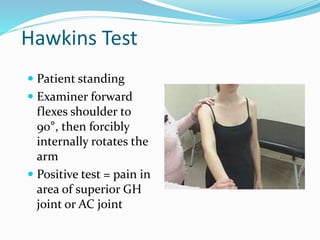
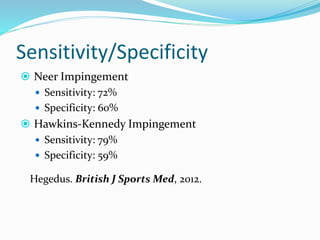
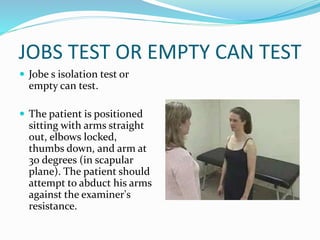
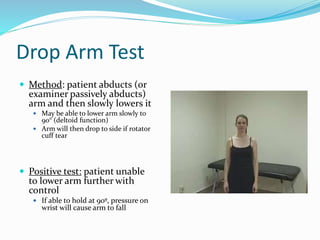
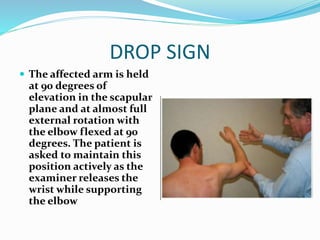
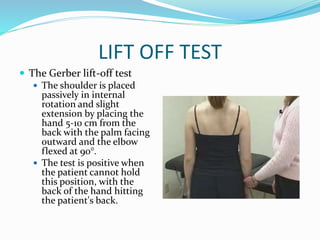
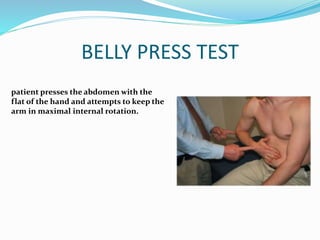
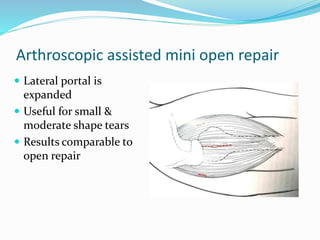
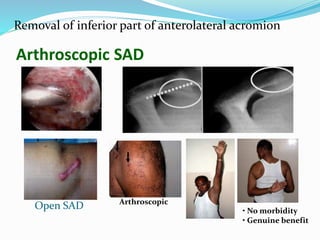
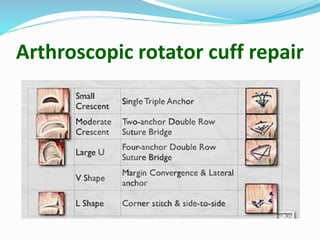
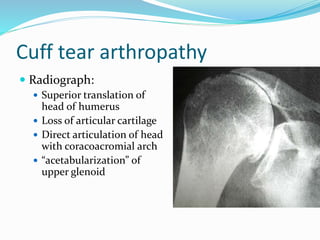
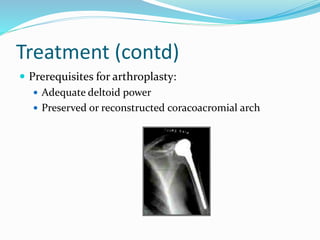
This document discusses the anatomy, biomechanics, causes, symptoms, diagnosis, and treatment of rotator cuff tears. It begins by introducing the rotator cuff muscles and their function in stabilizing the shoulder joint. Common causes of tears include impingement, trauma, aging, and ischemia. Symptoms include shoulder pain that is worsened with overhead activities. Diagnosis involves physical exam maneuvers like the Neer's and Hawkins tests as well as imaging like x-rays, ultrasound, CT, or MRI. Treatment ranges from rest, physical therapy, and injections for mild cases to surgical repair for larger or chronic tears if conservative measures fail.