Downloaded 801 times
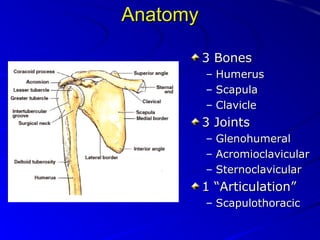
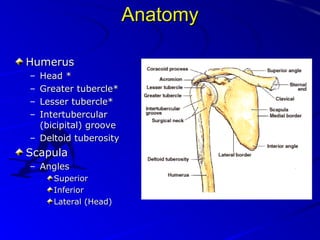
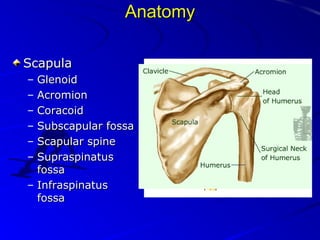
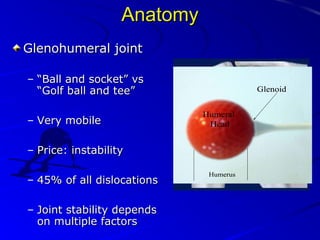
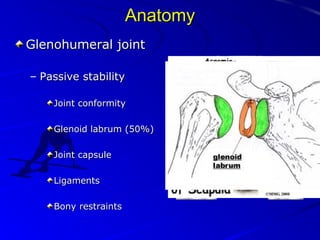
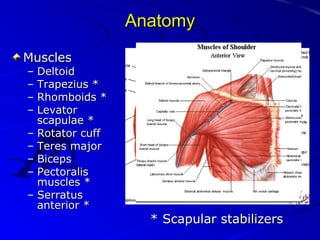
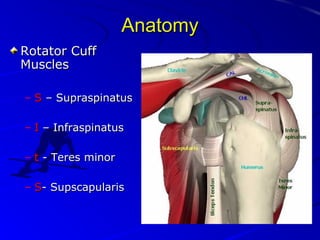
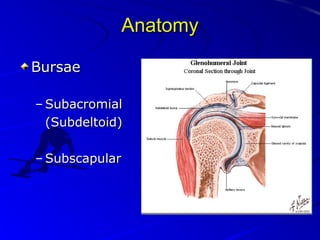
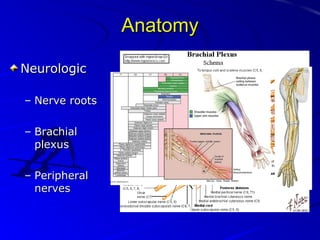
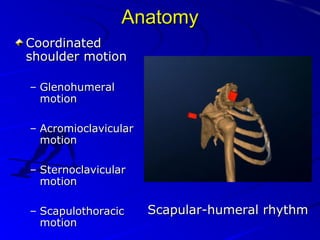
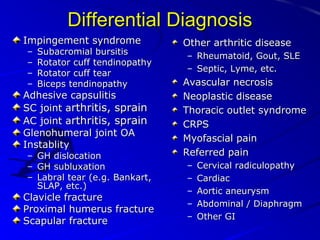

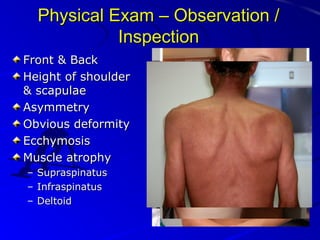
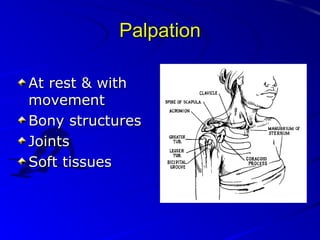
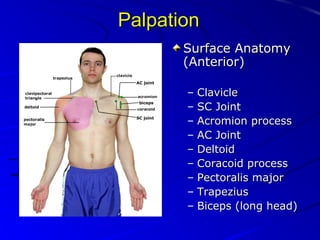
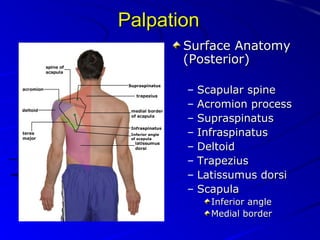
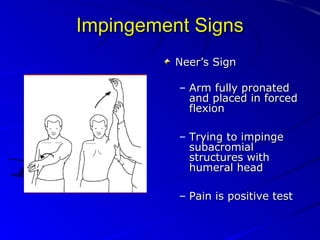
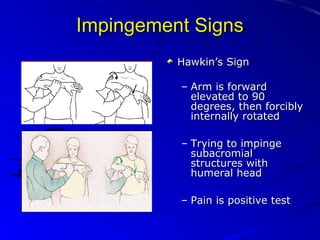
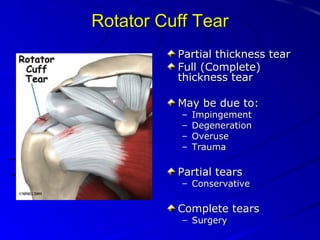
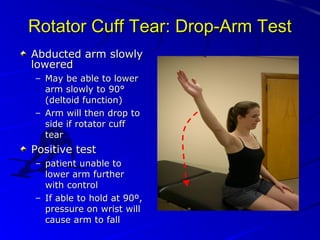
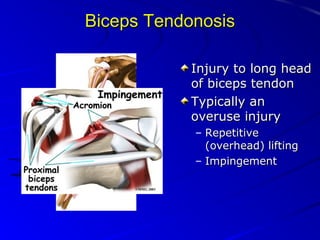

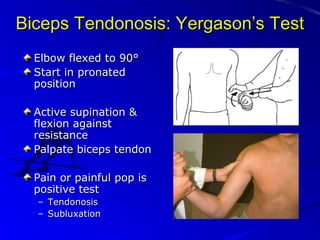
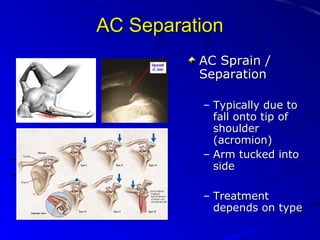
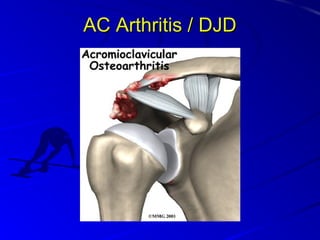
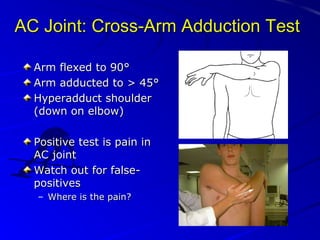
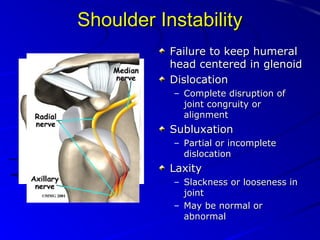
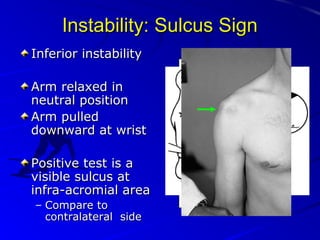
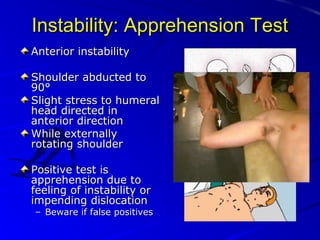
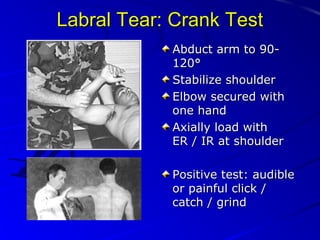
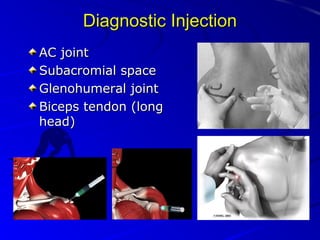
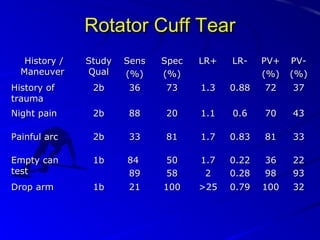
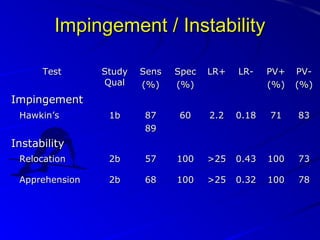
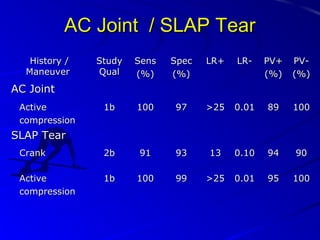
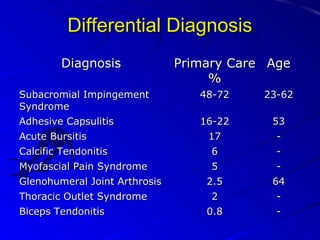

This document provides an overview of performing a physical examination of the shoulder. It begins with reviewing the relevant anatomy of the shoulder, including the bones, joints, muscles, and bursae. Common differential diagnoses for shoulder pain are listed. The document then details how to perform the physical examination, including inspection, palpation, range of motion testing, strength testing, and special tests. It provides descriptions of how to perform tests for conditions like impingement, rotator cuff tears, biceps tendonitis, AC joint injuries, instability, and labral tears. Tables at the end summarize the sensitivity, specificity, and likelihood ratios of various history and physical exam maneuvers for diagnosing various shoulder conditions.
































































![Shoulder_joint_and_applied_aspects[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/shoulderjointandappliedaspects1-240425164911-e75cbd49-thumbnail.jpg?width=640&height=640&fit=bounds)






















