The document provides information on examining the shoulder joint, including:
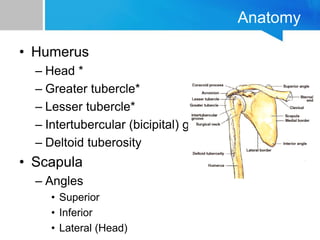
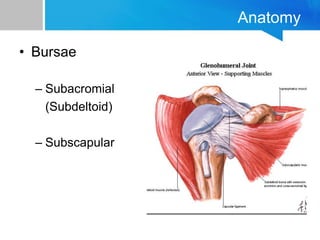
1) It describes the anatomy of the shoulder joint which involves three bones and three joints.
2) Common shoulder injuries include rotator cuff problems, impingement syndrome, and athletic injuries.
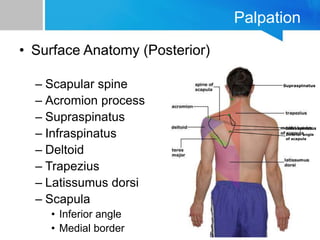
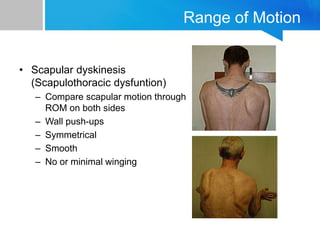
3) The physical exam involves inspection for atrophy or deformity, palpation of bony landmarks and soft tissues, and assessment of range of motion and strength.
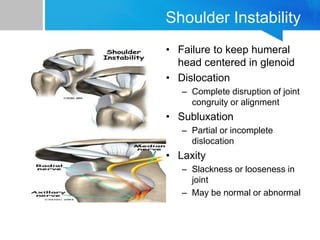
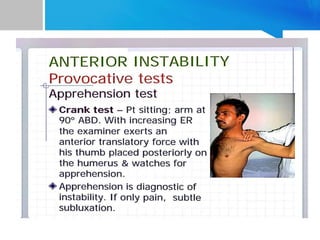
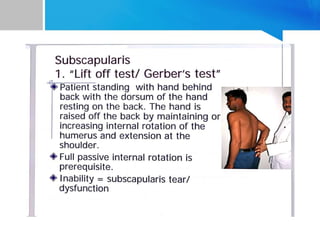
4) Special tests examine for issues like instability, impingement, rotator cuff tears, biceps problems, and AC joint pathology.