This document provides an overview of the physical examination of the shoulder, including:
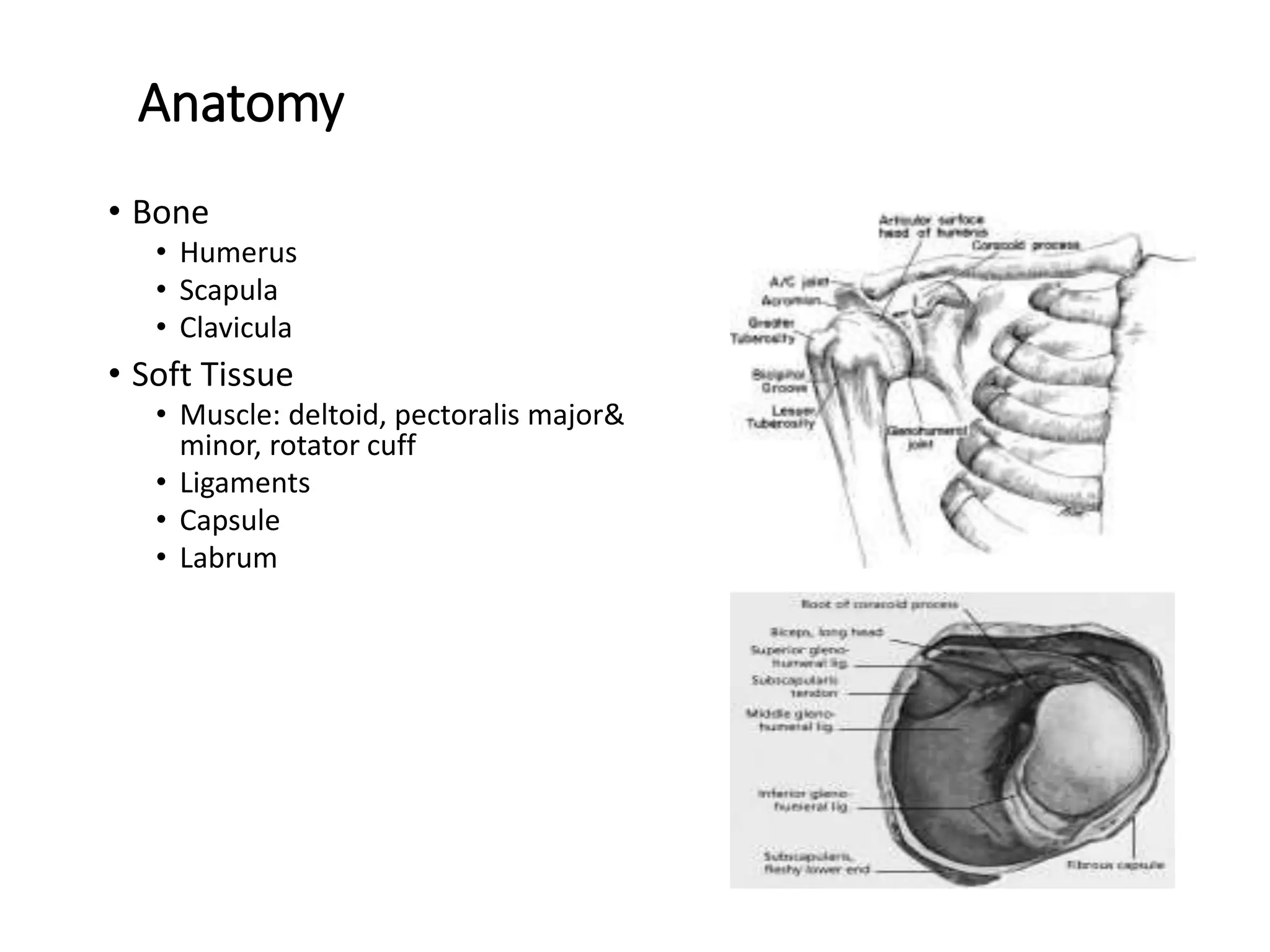
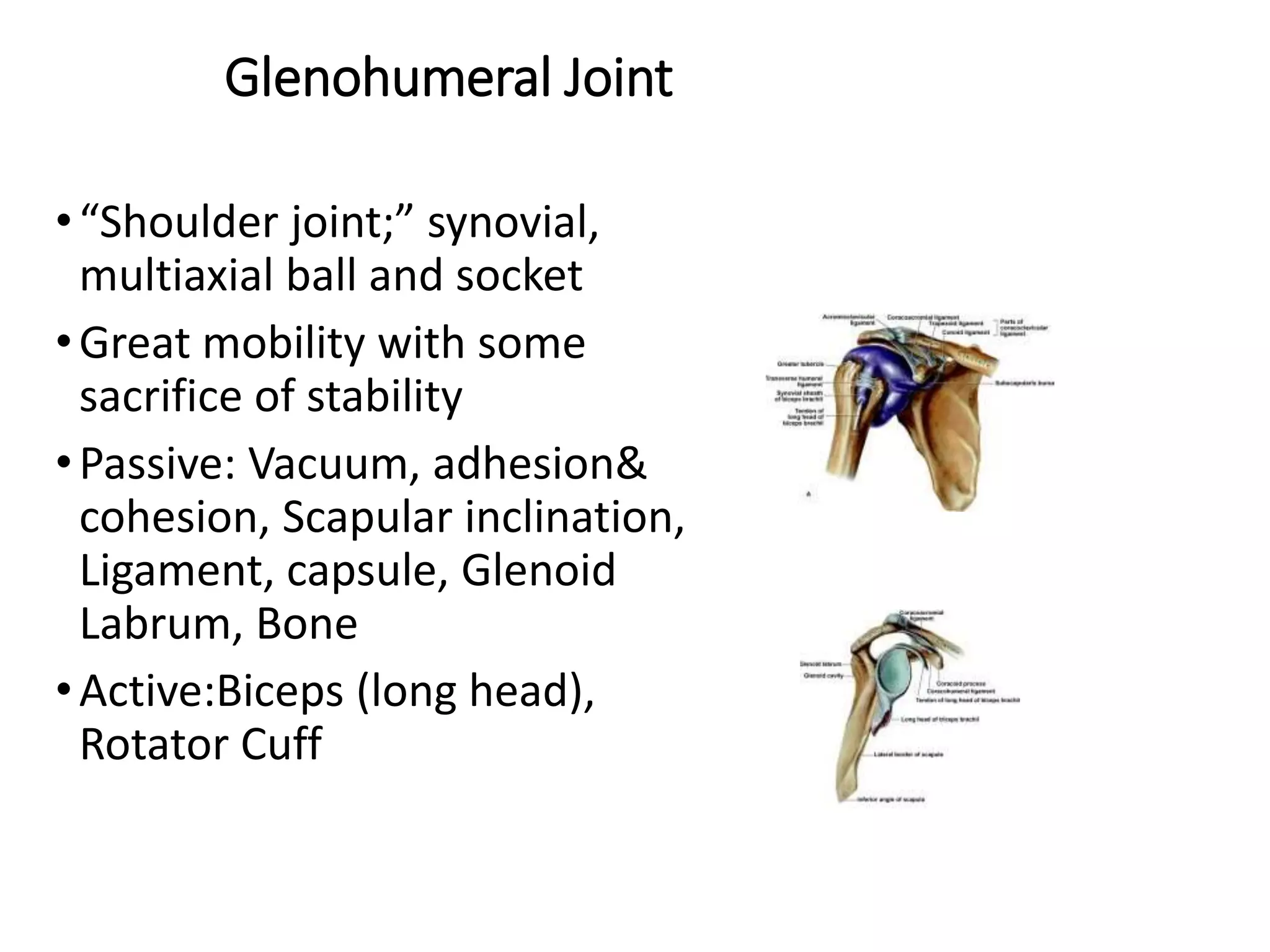
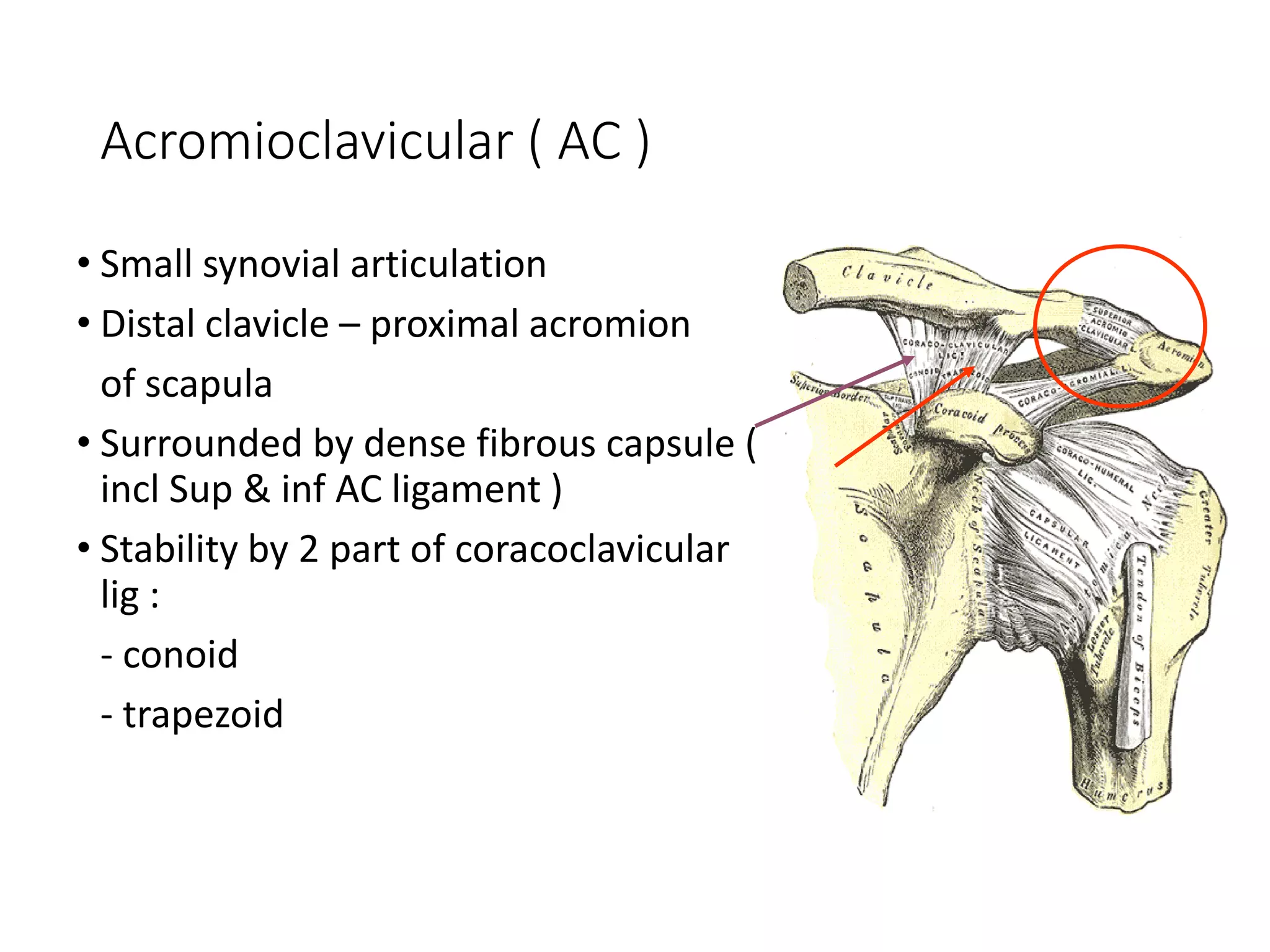
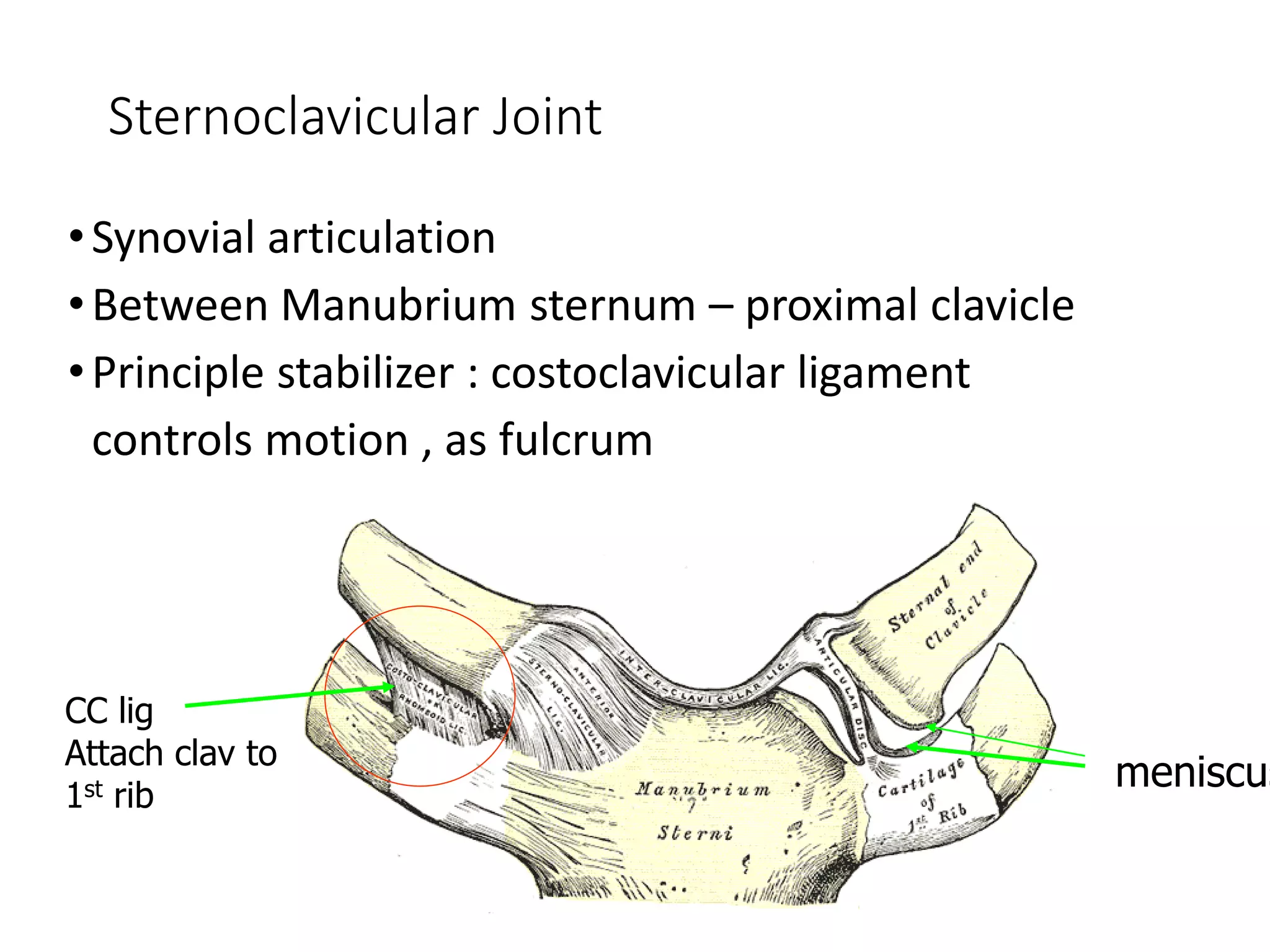
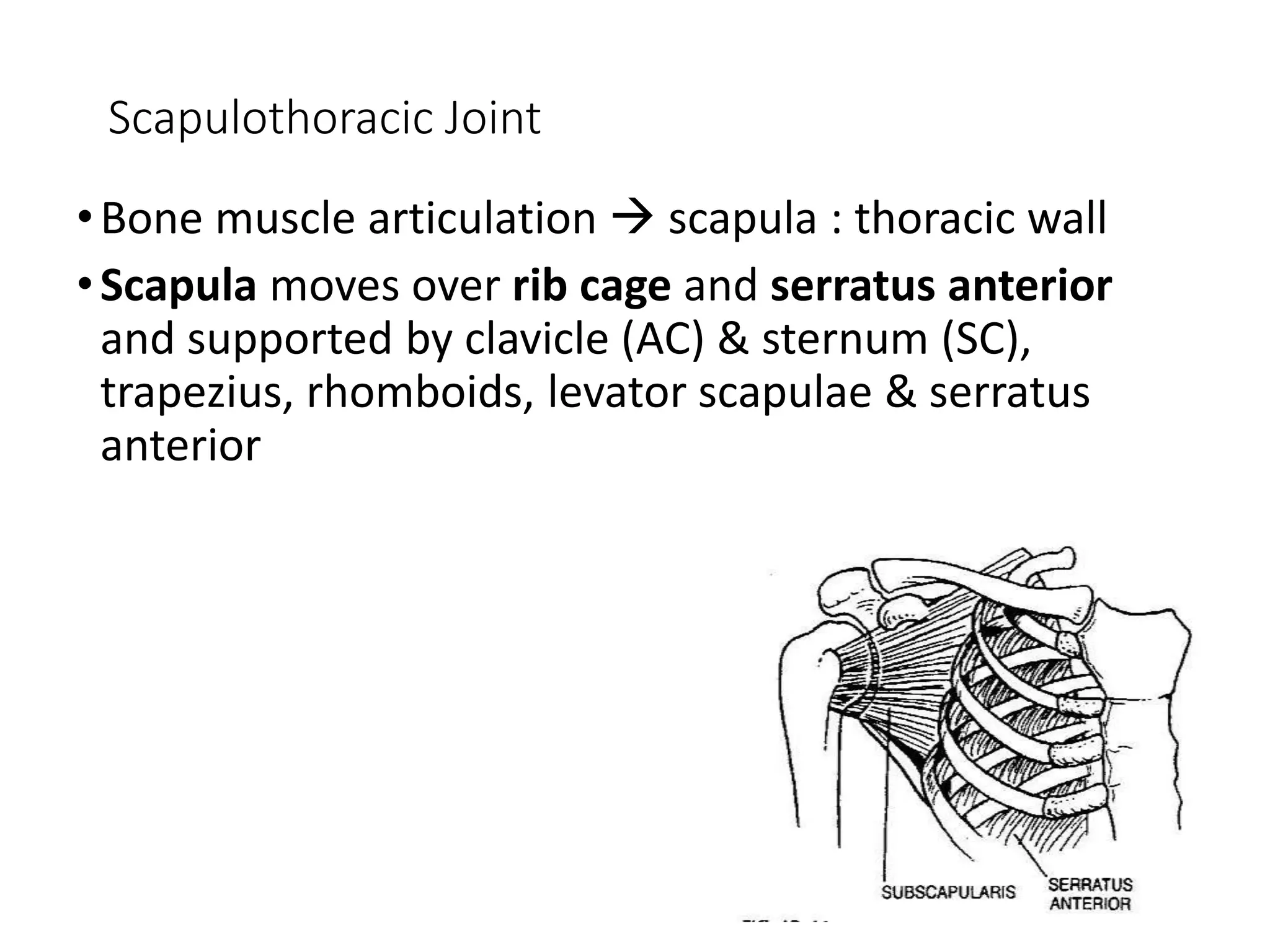
1. The anatomy of the shoulder including bones, muscles, and ligaments.
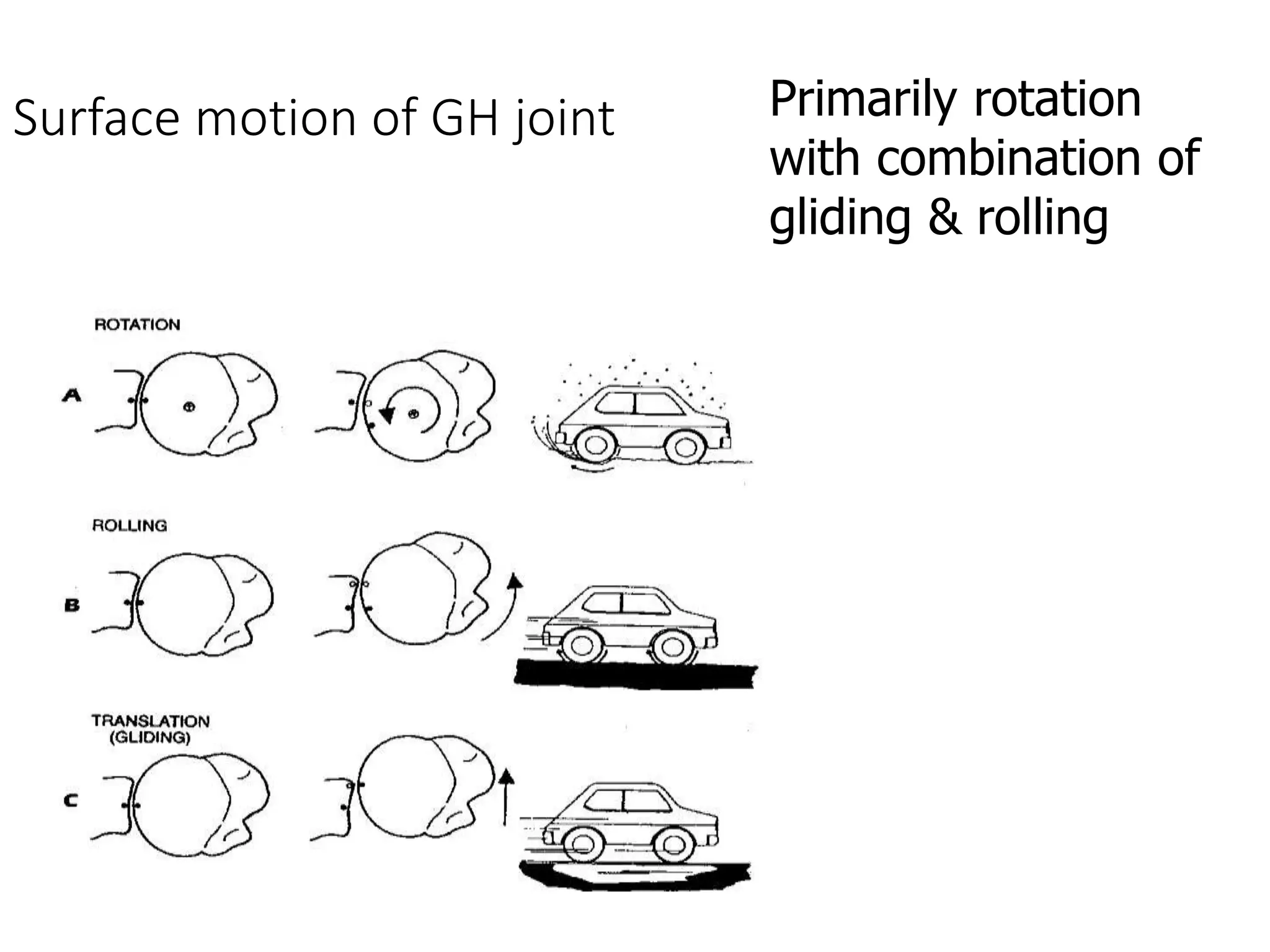
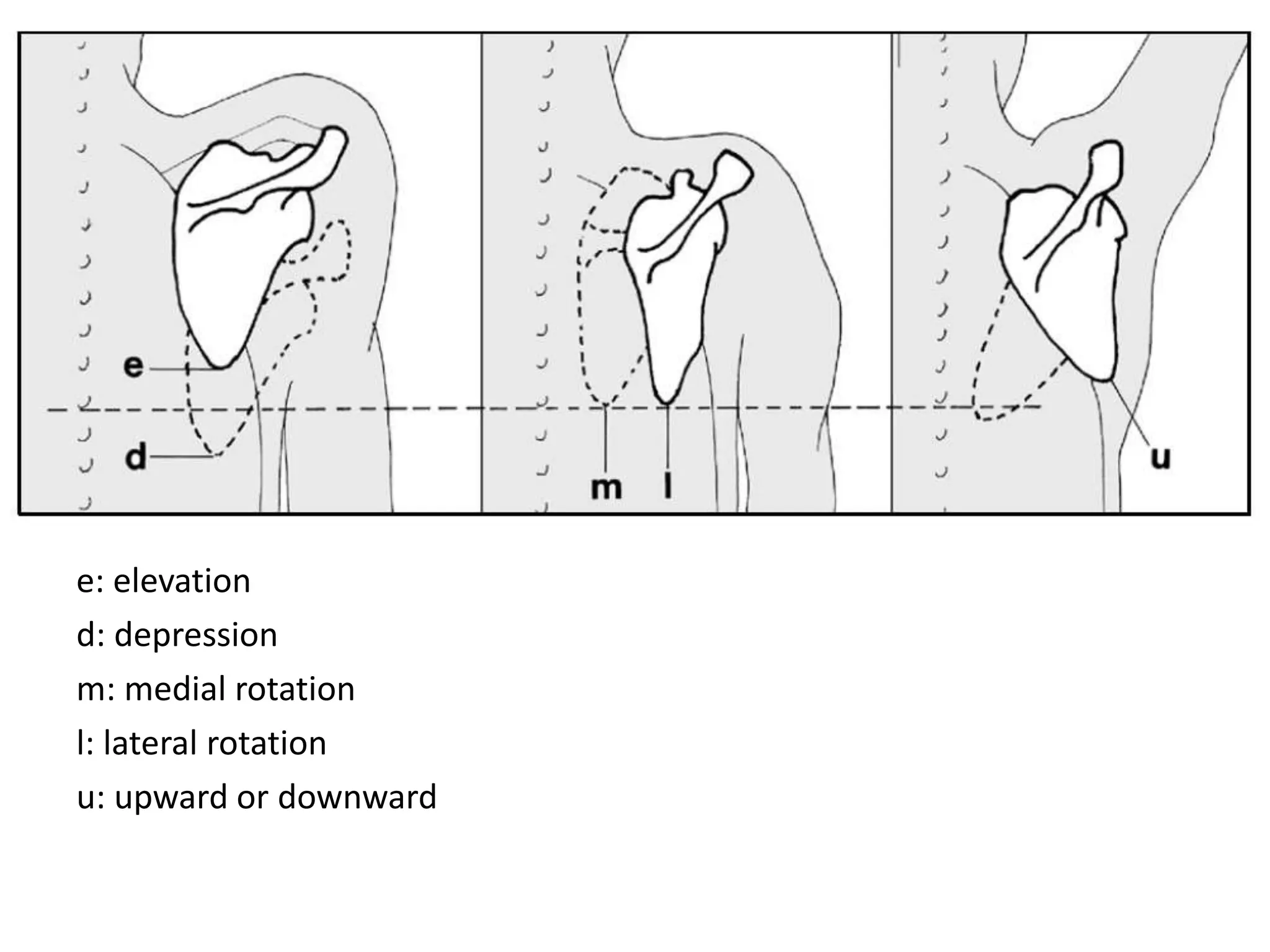
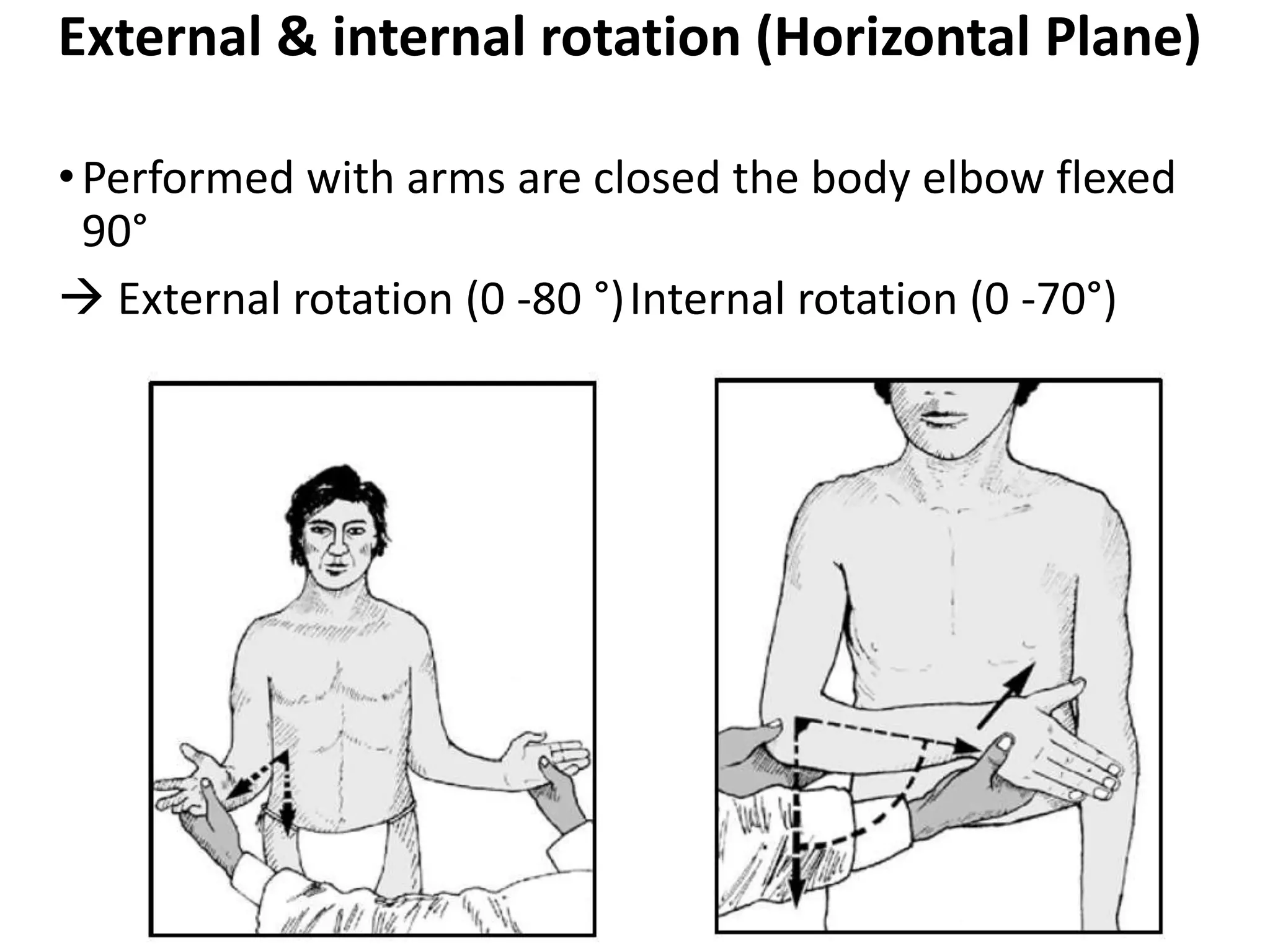
2. Descriptions of various motions of the shoulder like flexion, extension, abduction, and rotation.
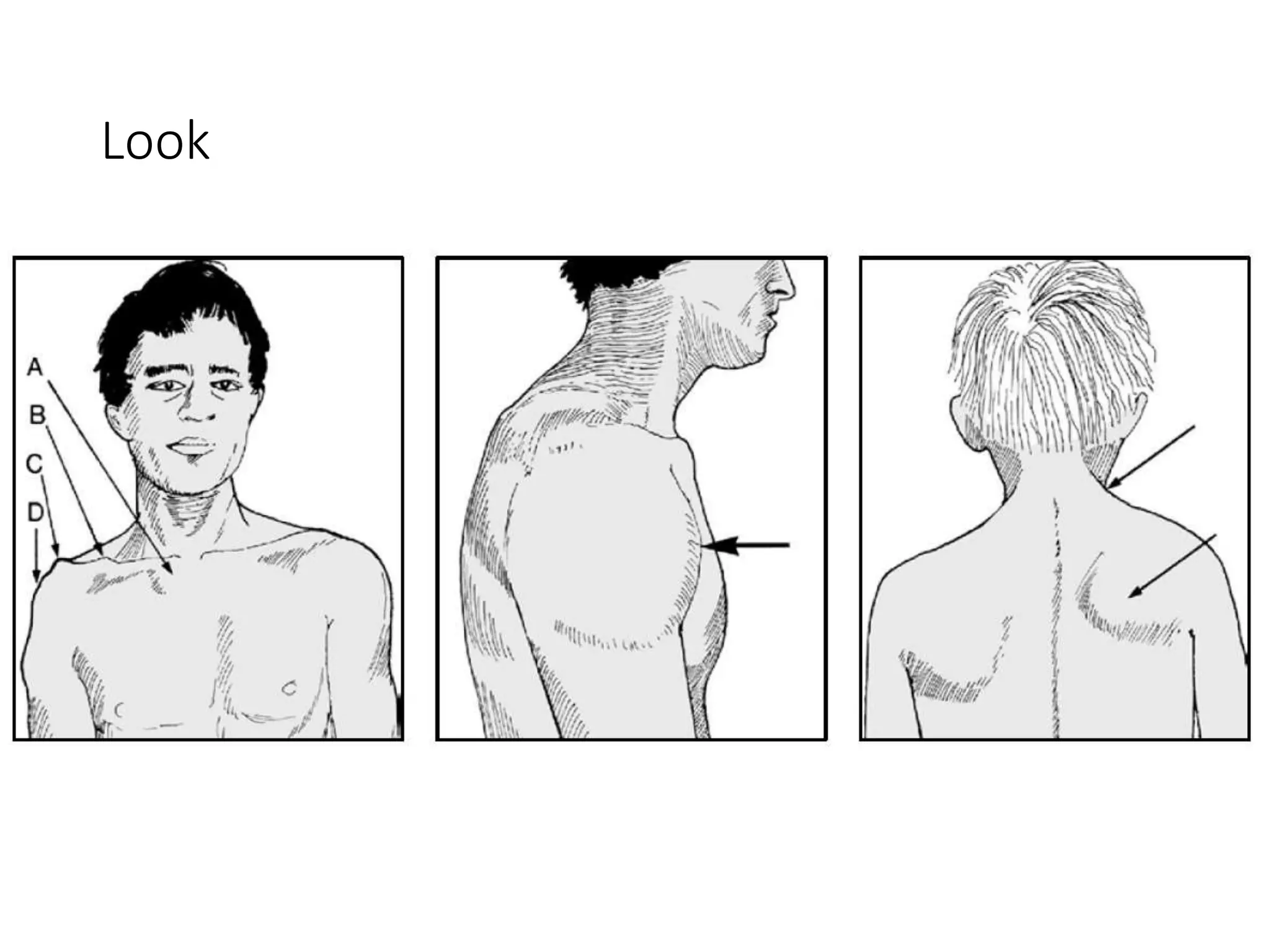
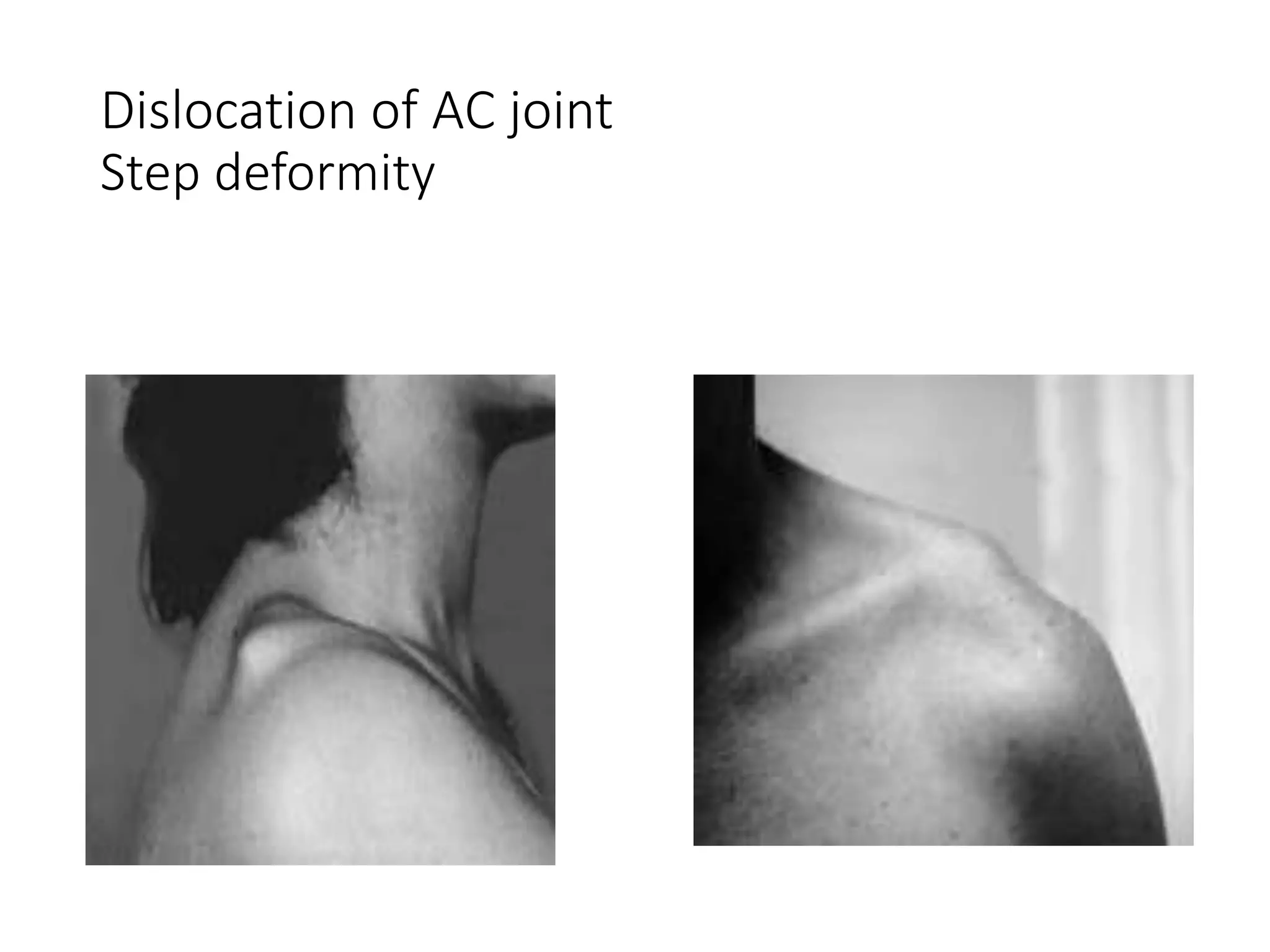
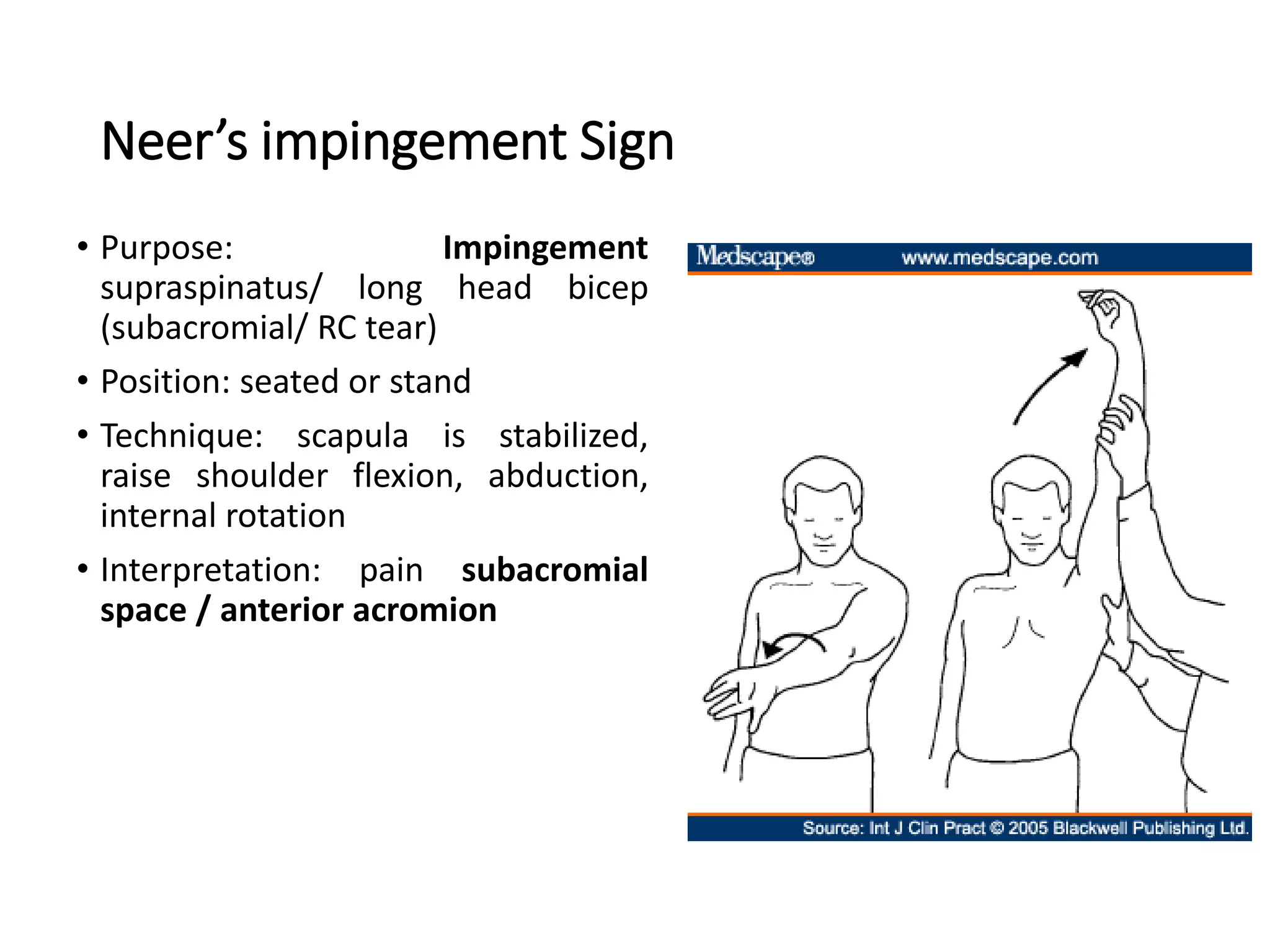
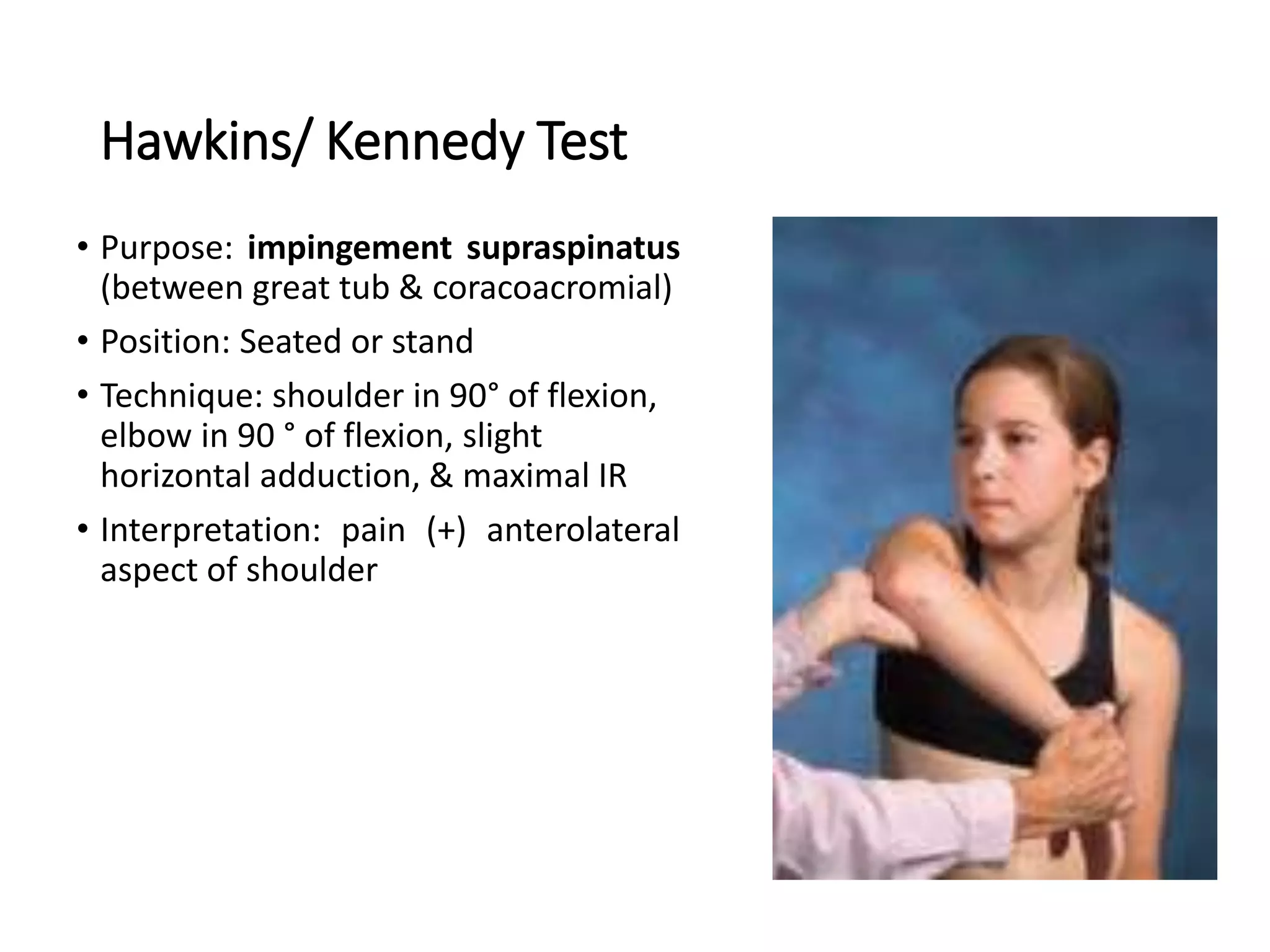
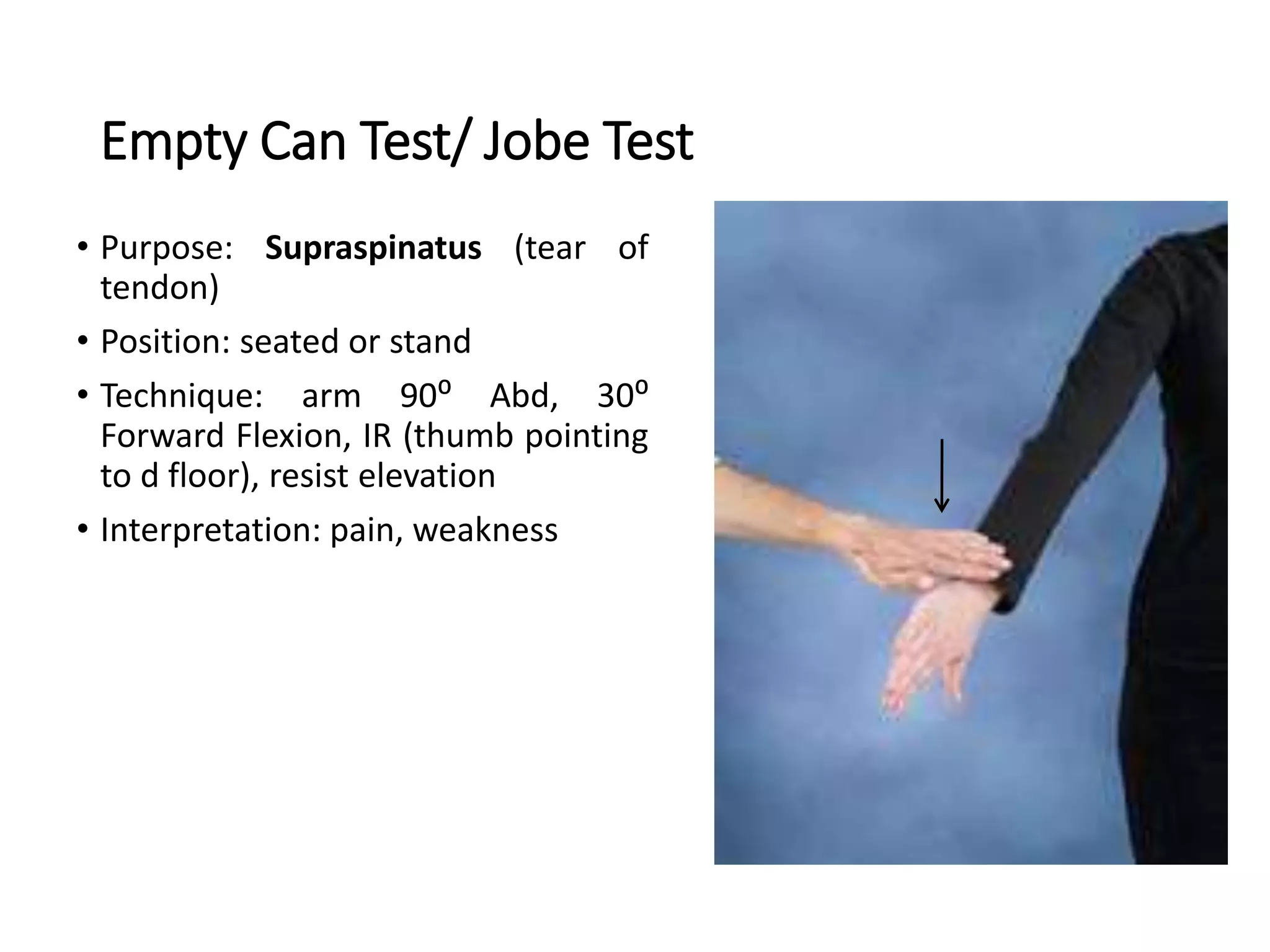
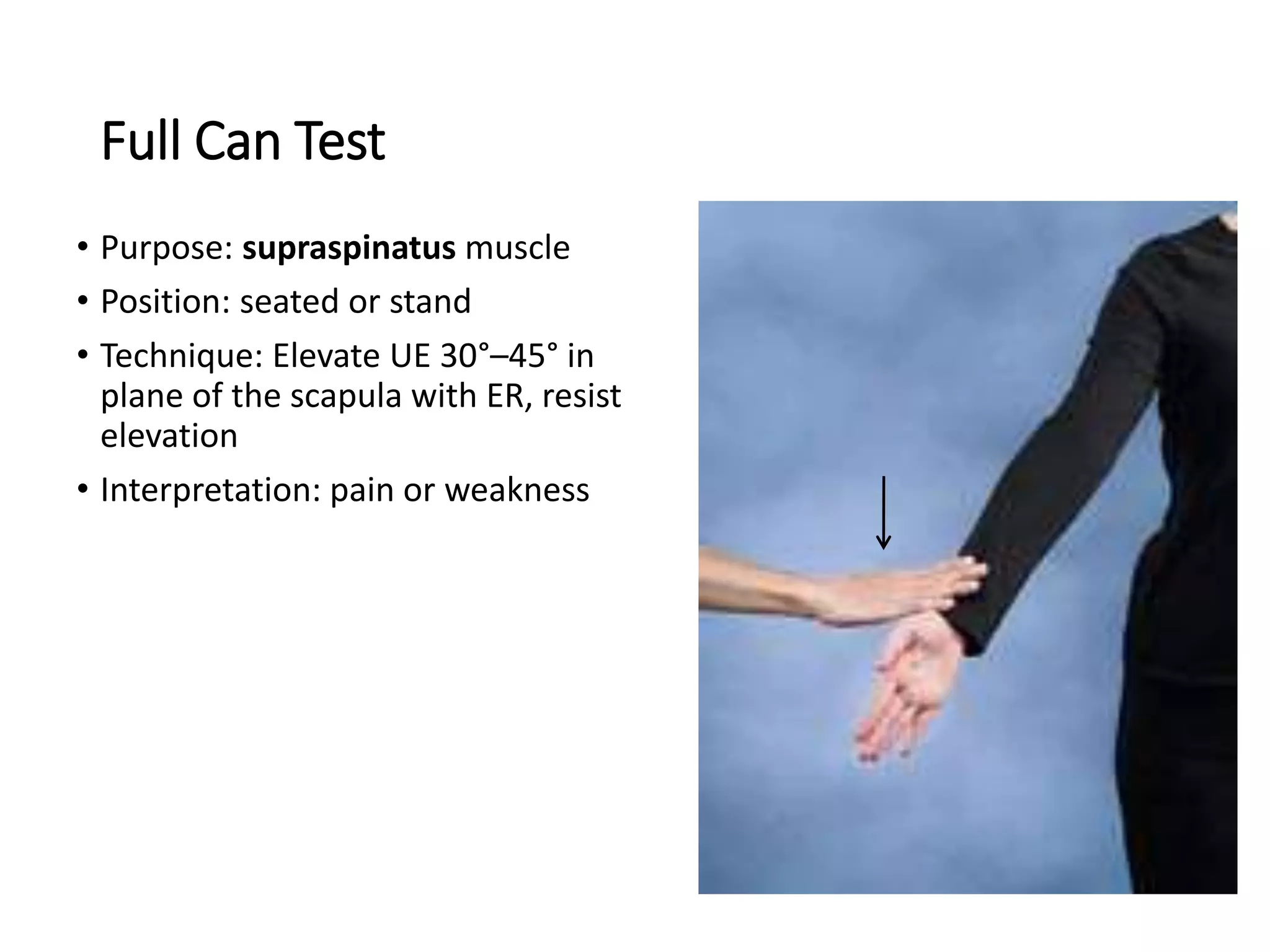
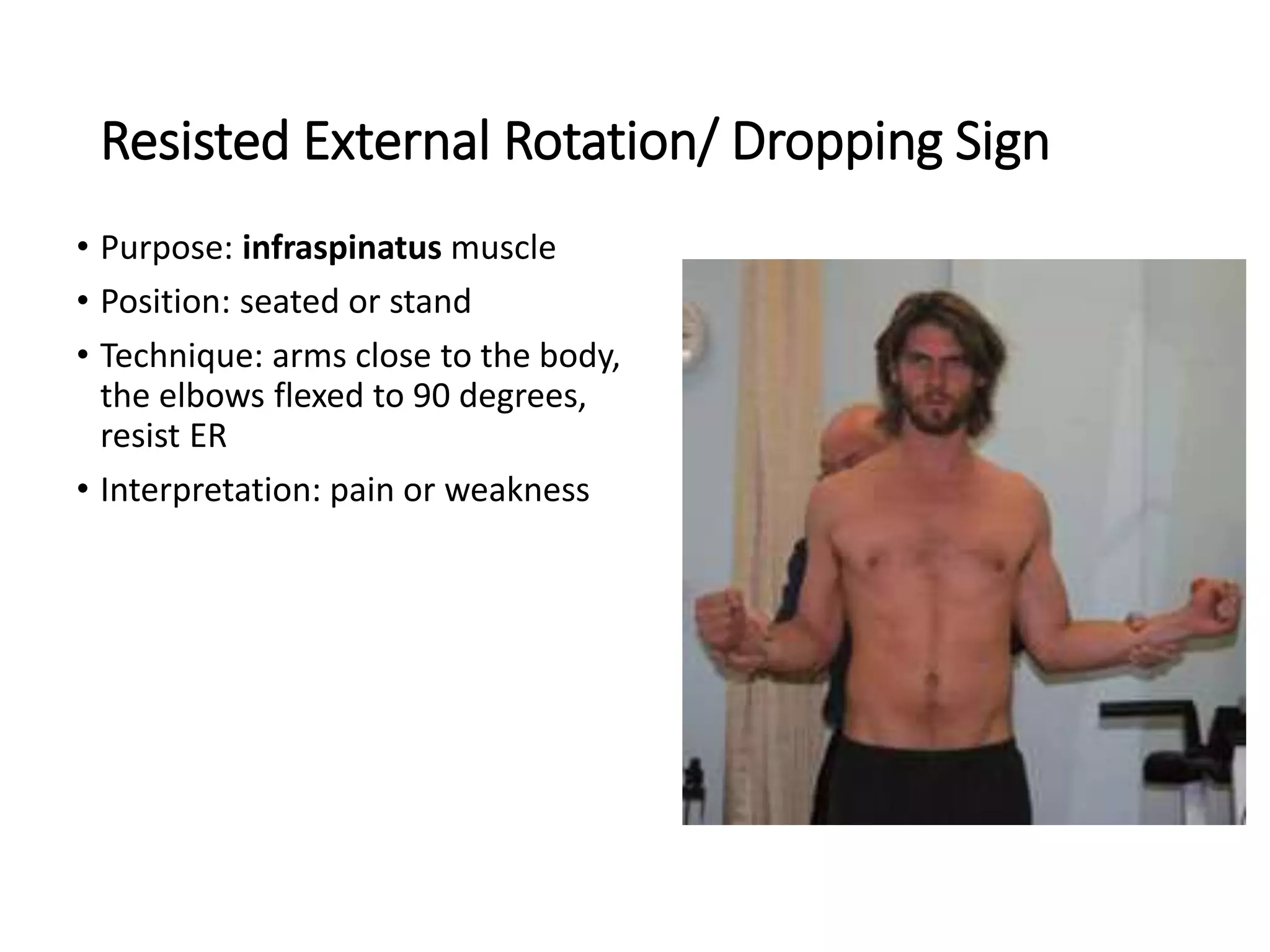
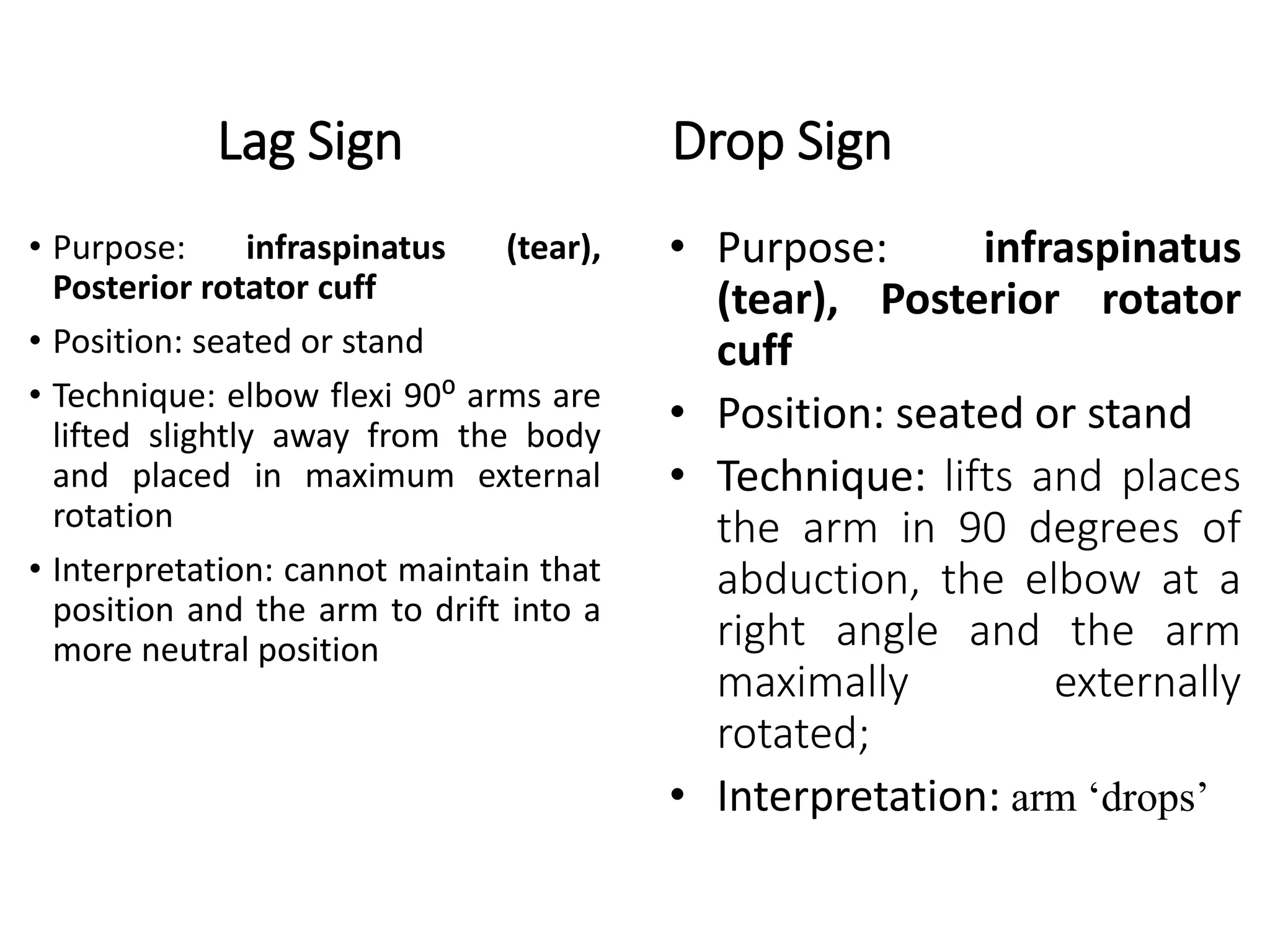
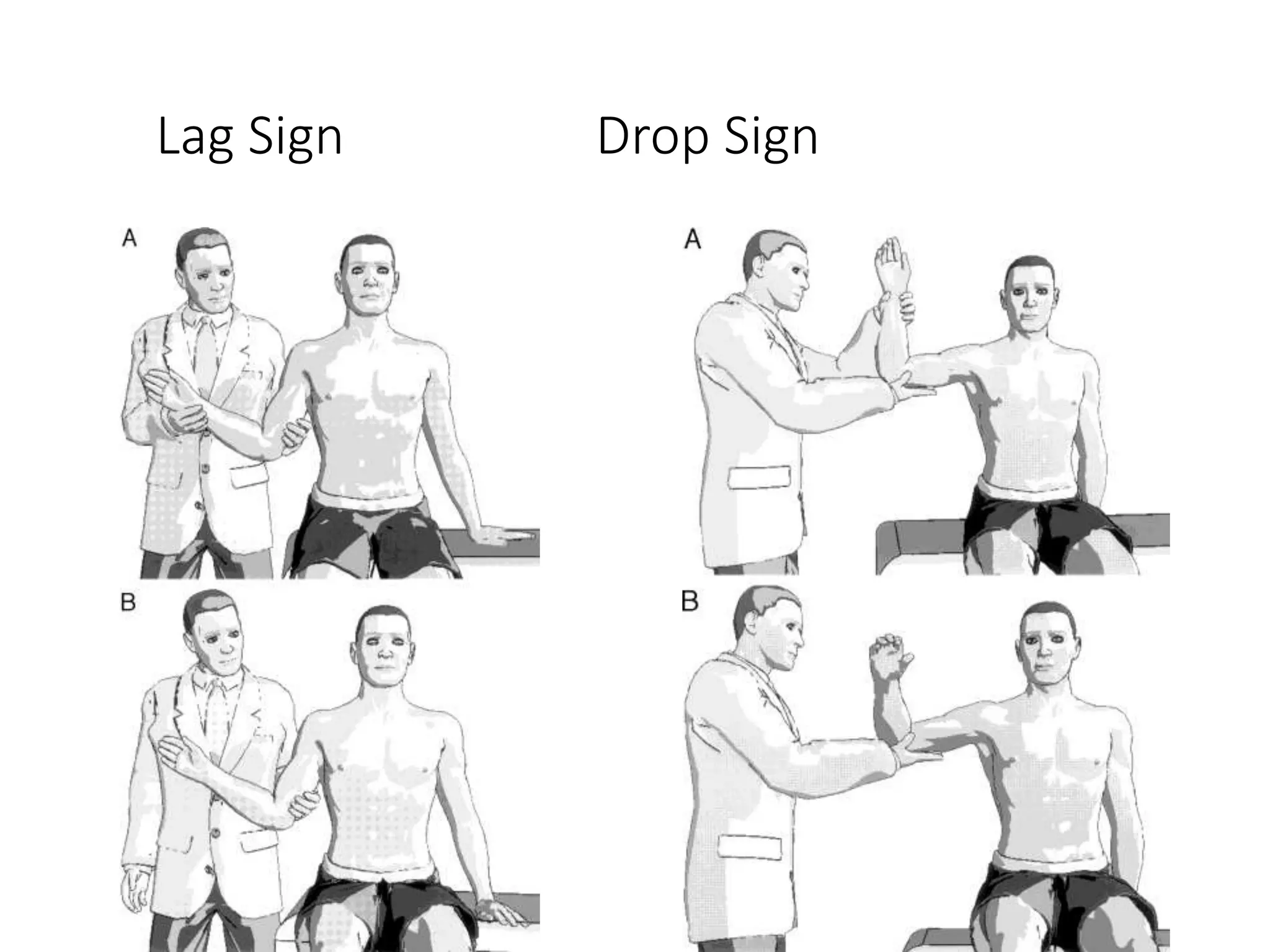
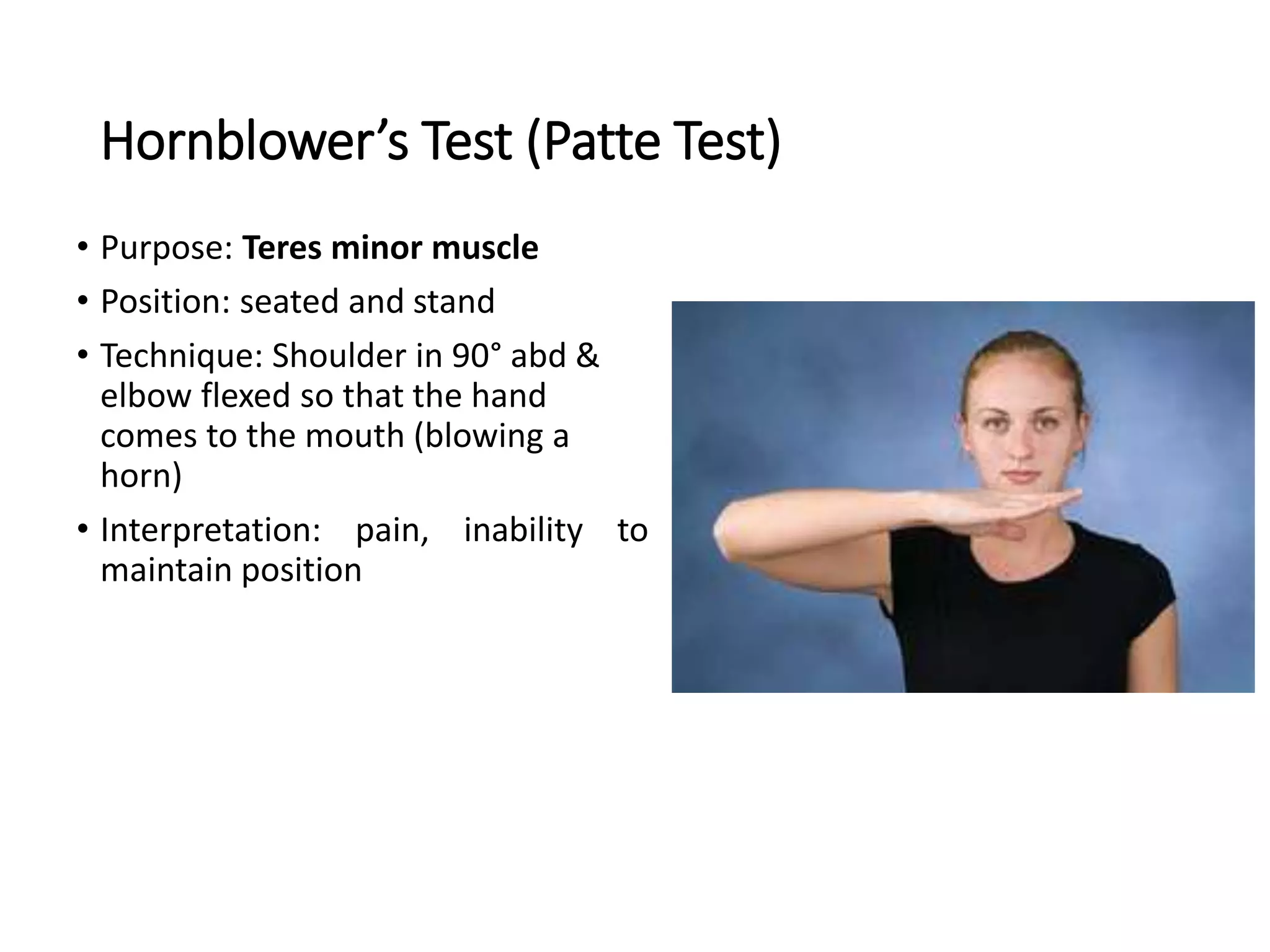
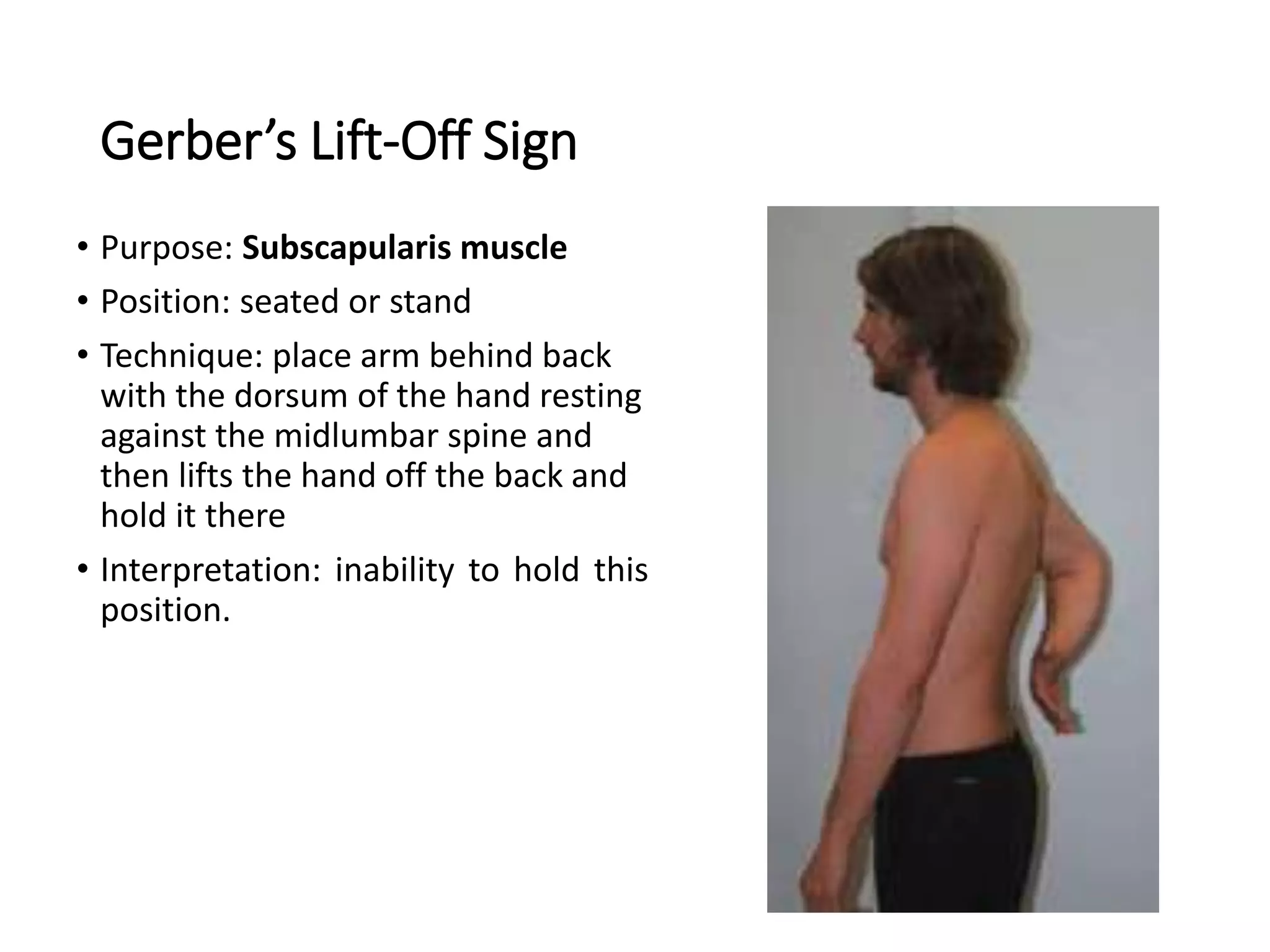
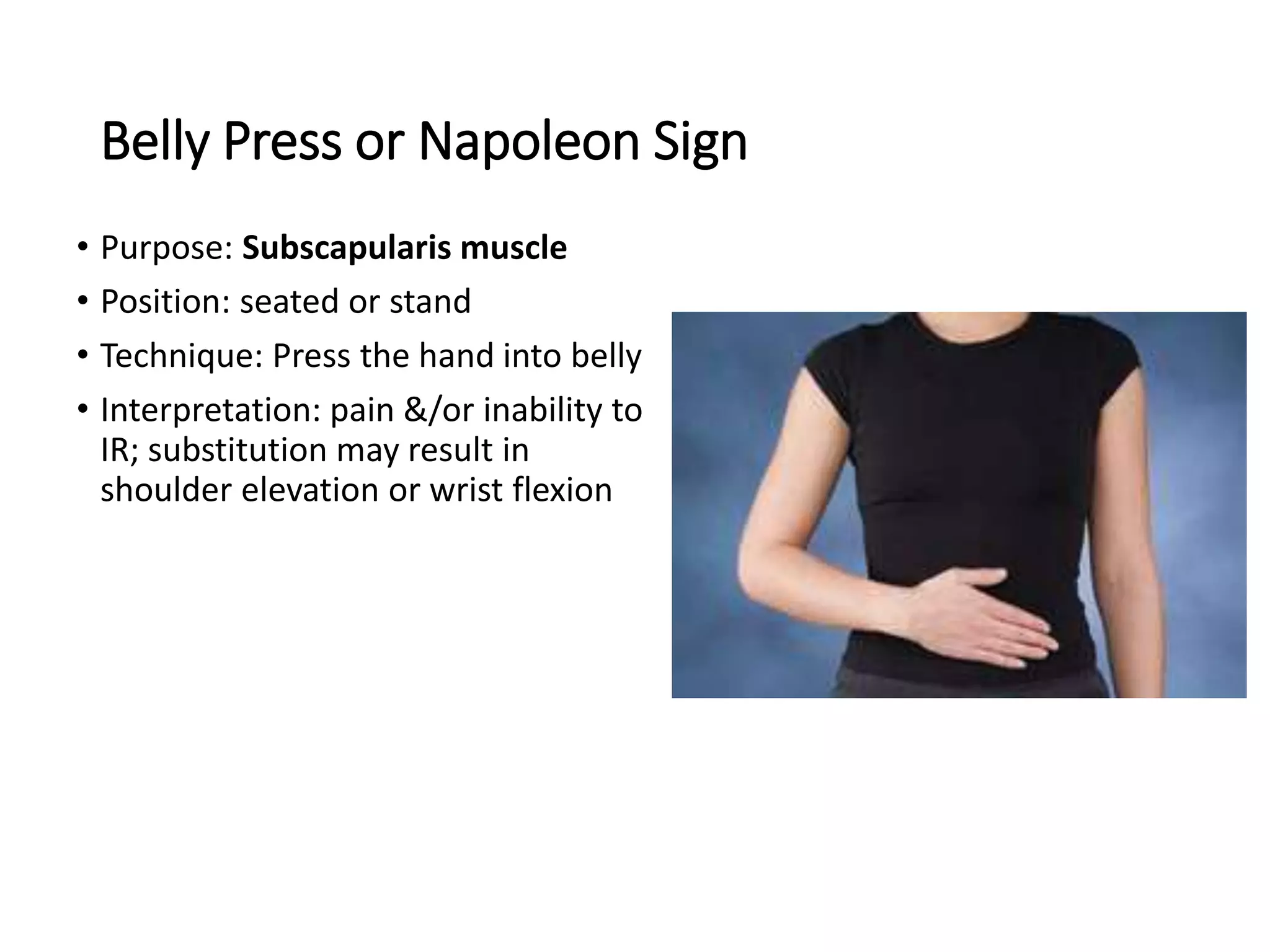
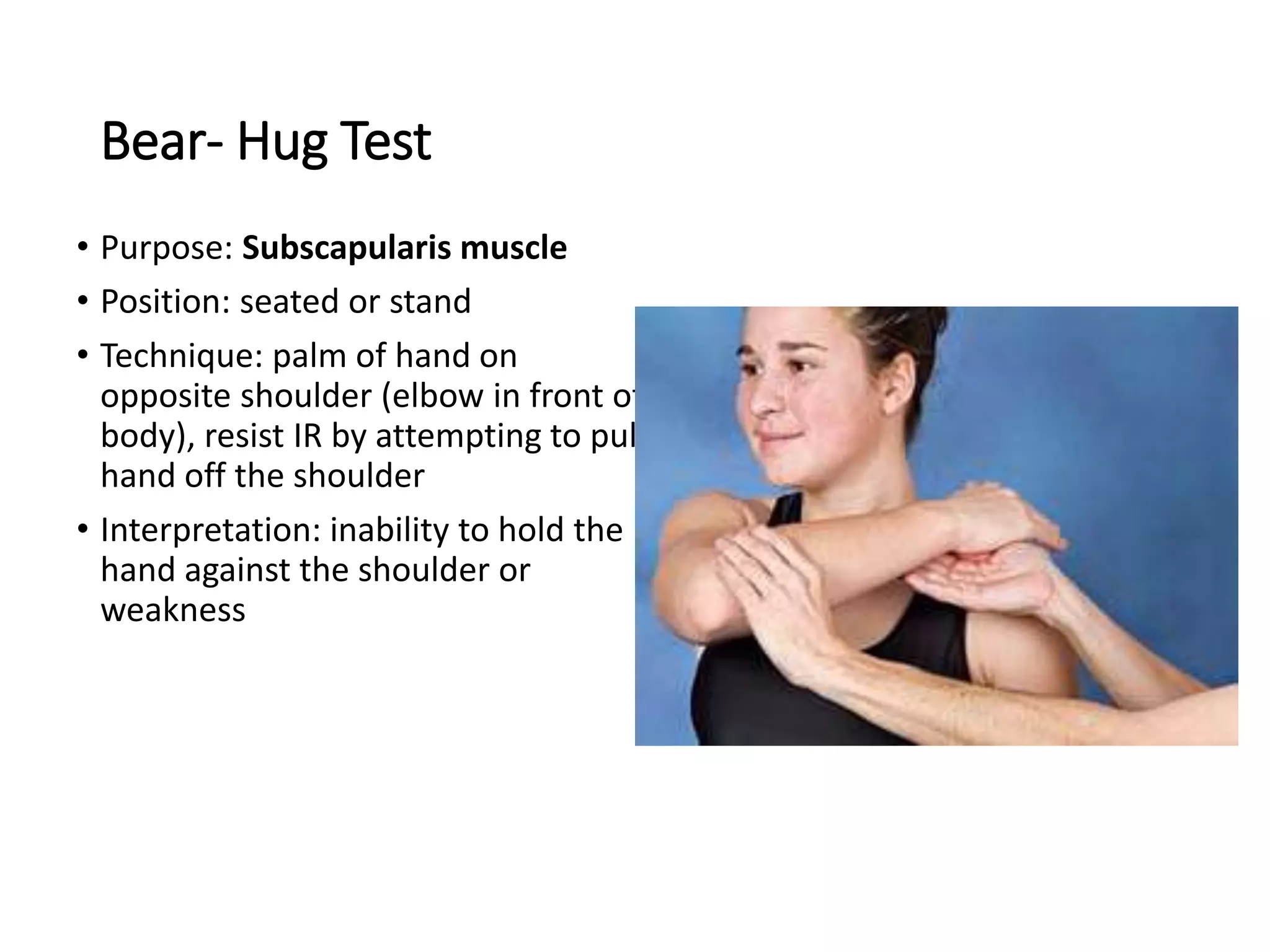
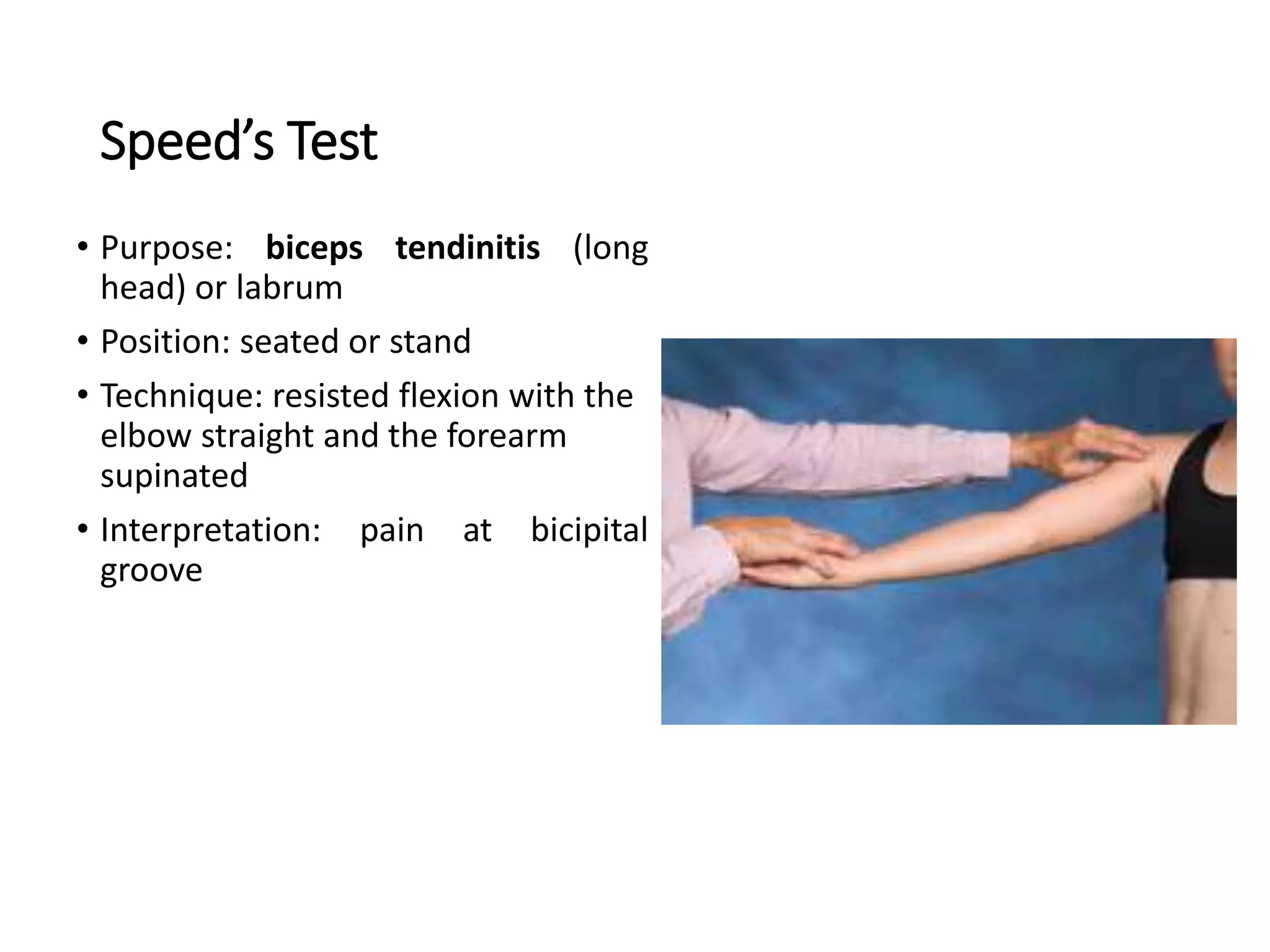
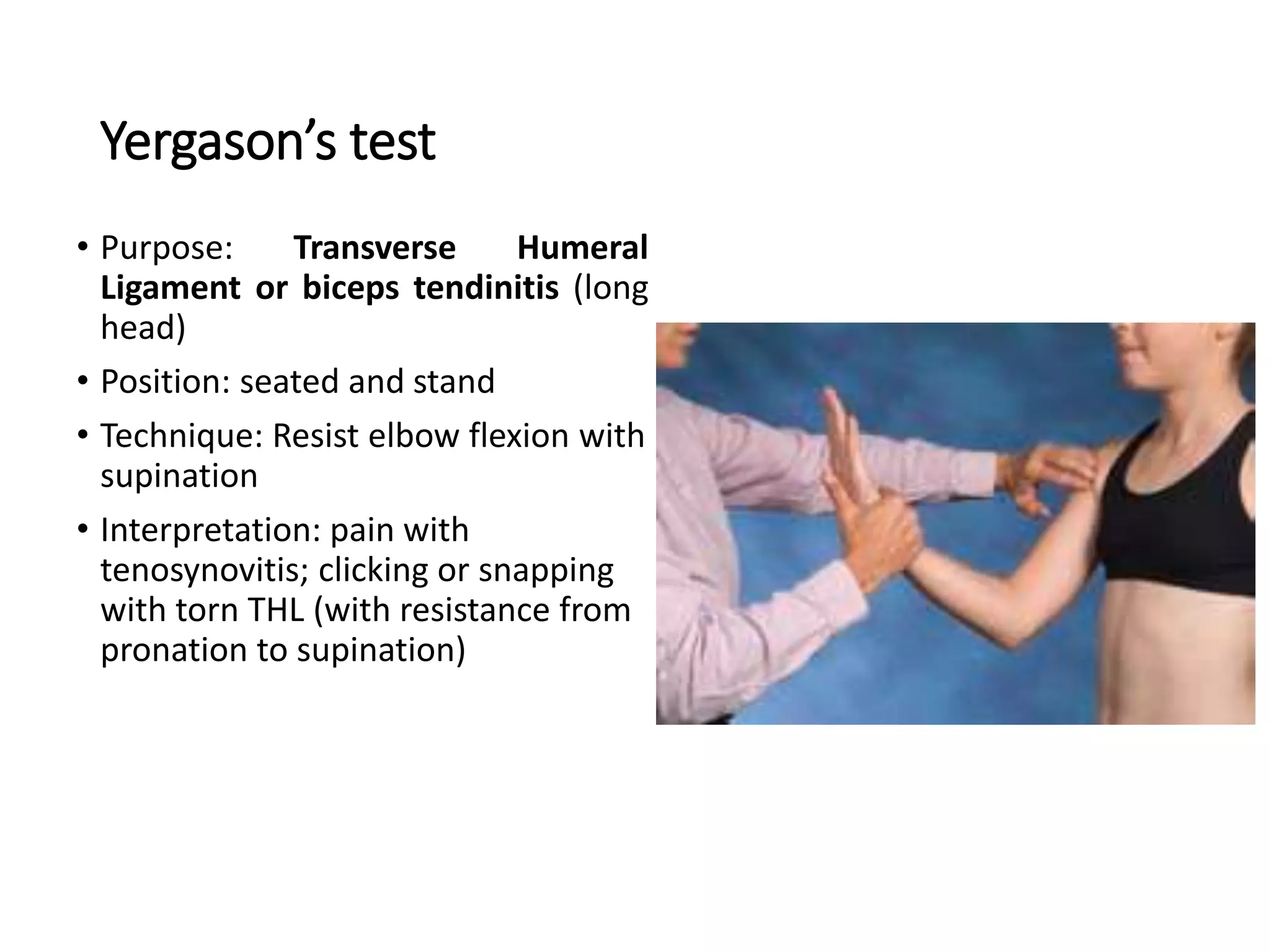
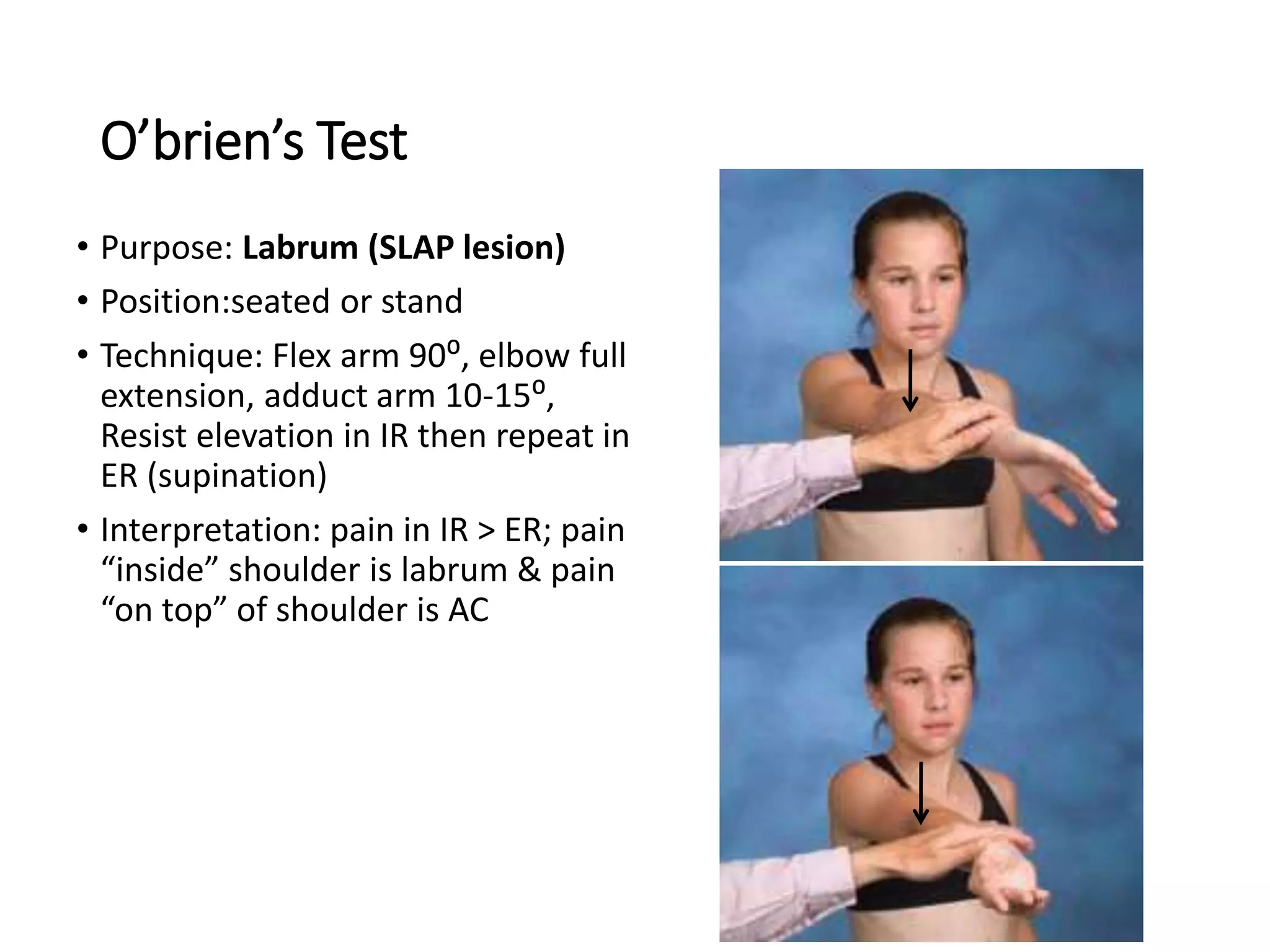
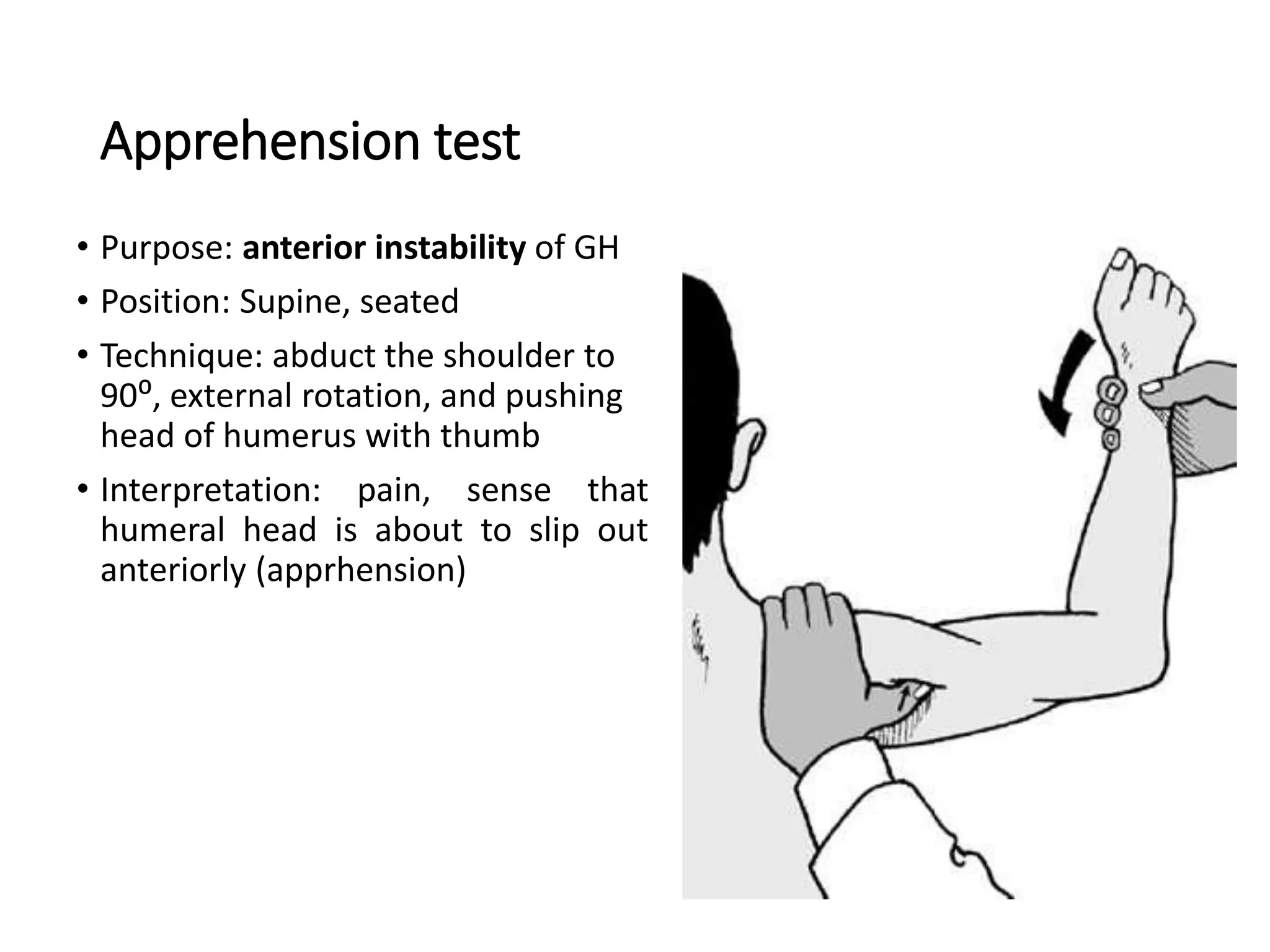
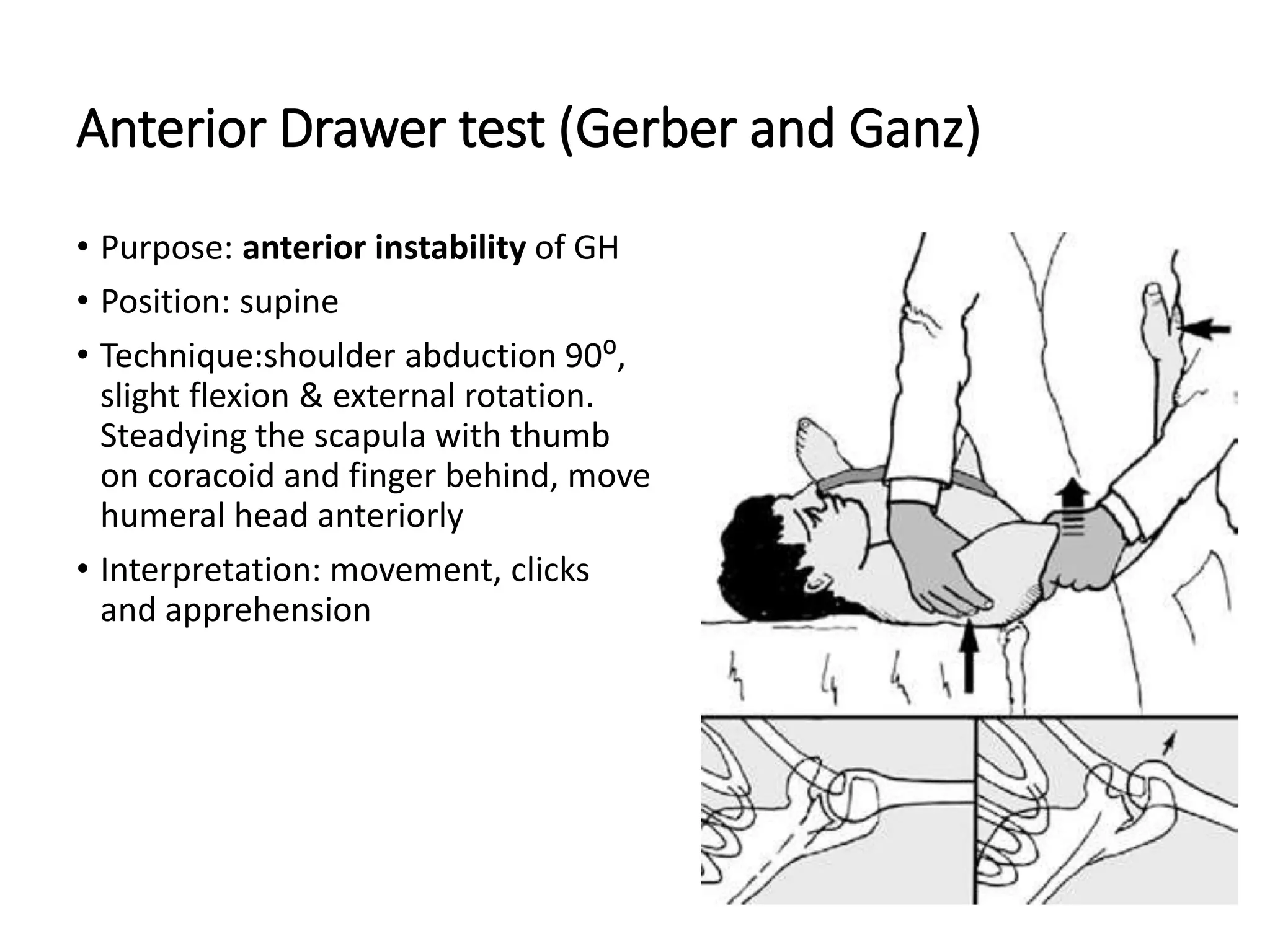
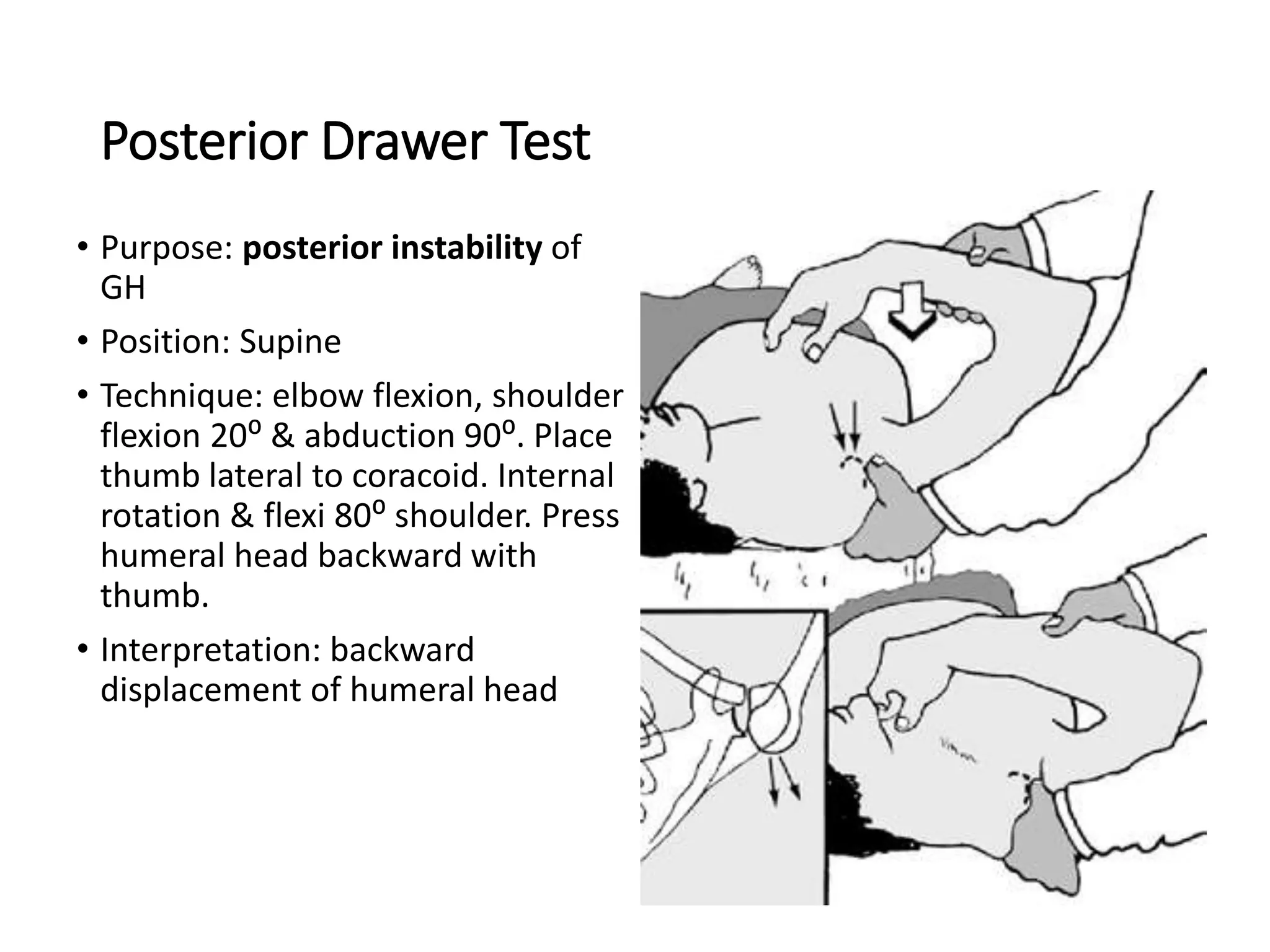
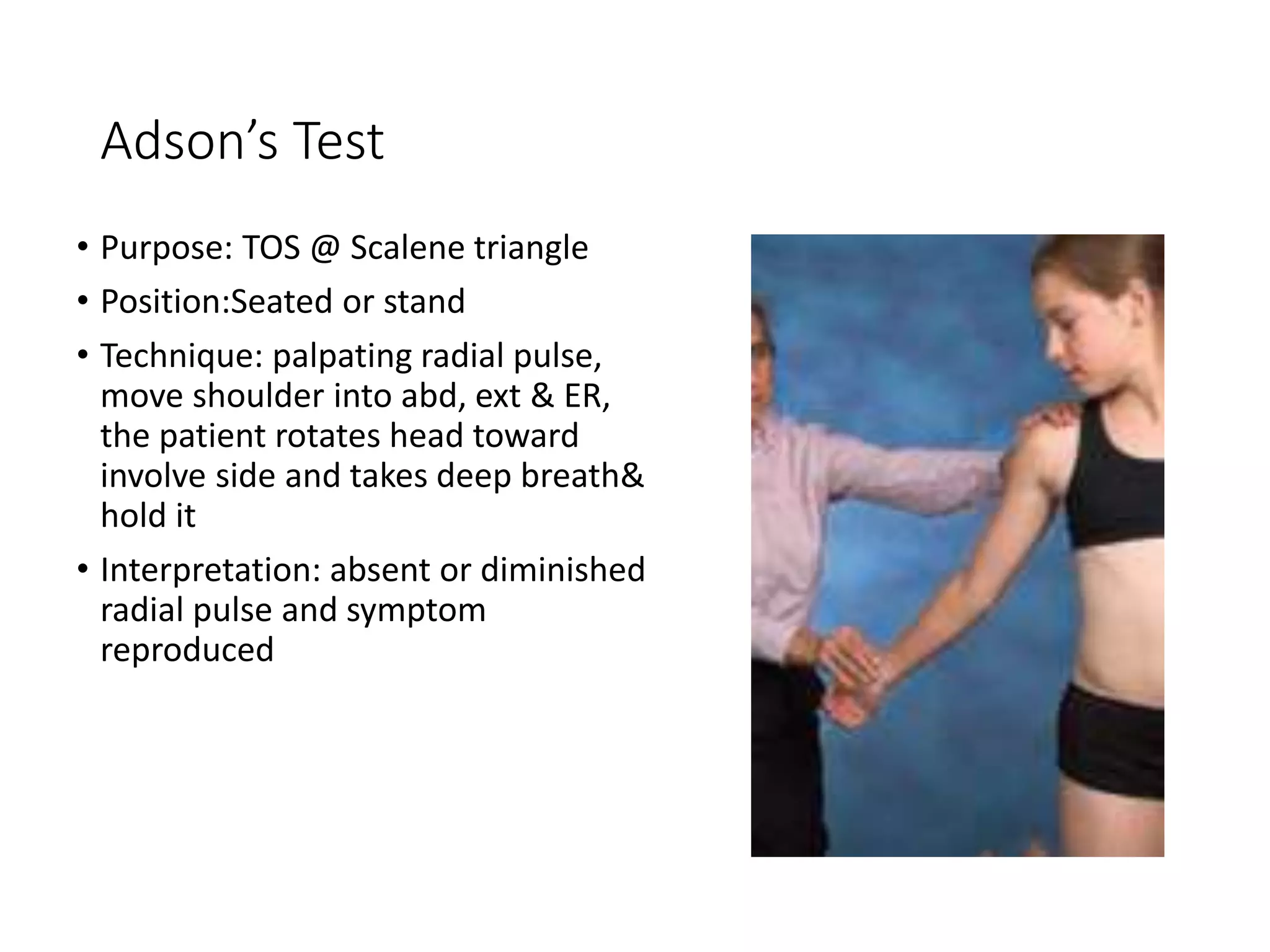
3. Details on clinical assessment including inspection, palpation, and special tests to evaluate the shoulder for issues like impingement, instability, and thoracic outlet syndrome. Special tests evaluate specific muscles, ligaments, and structures of the shoulder.


































































![Shoulder_joint_and_applied_aspects[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/shoulderjointandappliedaspects1-240425164911-e75cbd49-thumbnail.jpg?width=640&height=640&fit=bounds)























