Downloaded 484 times




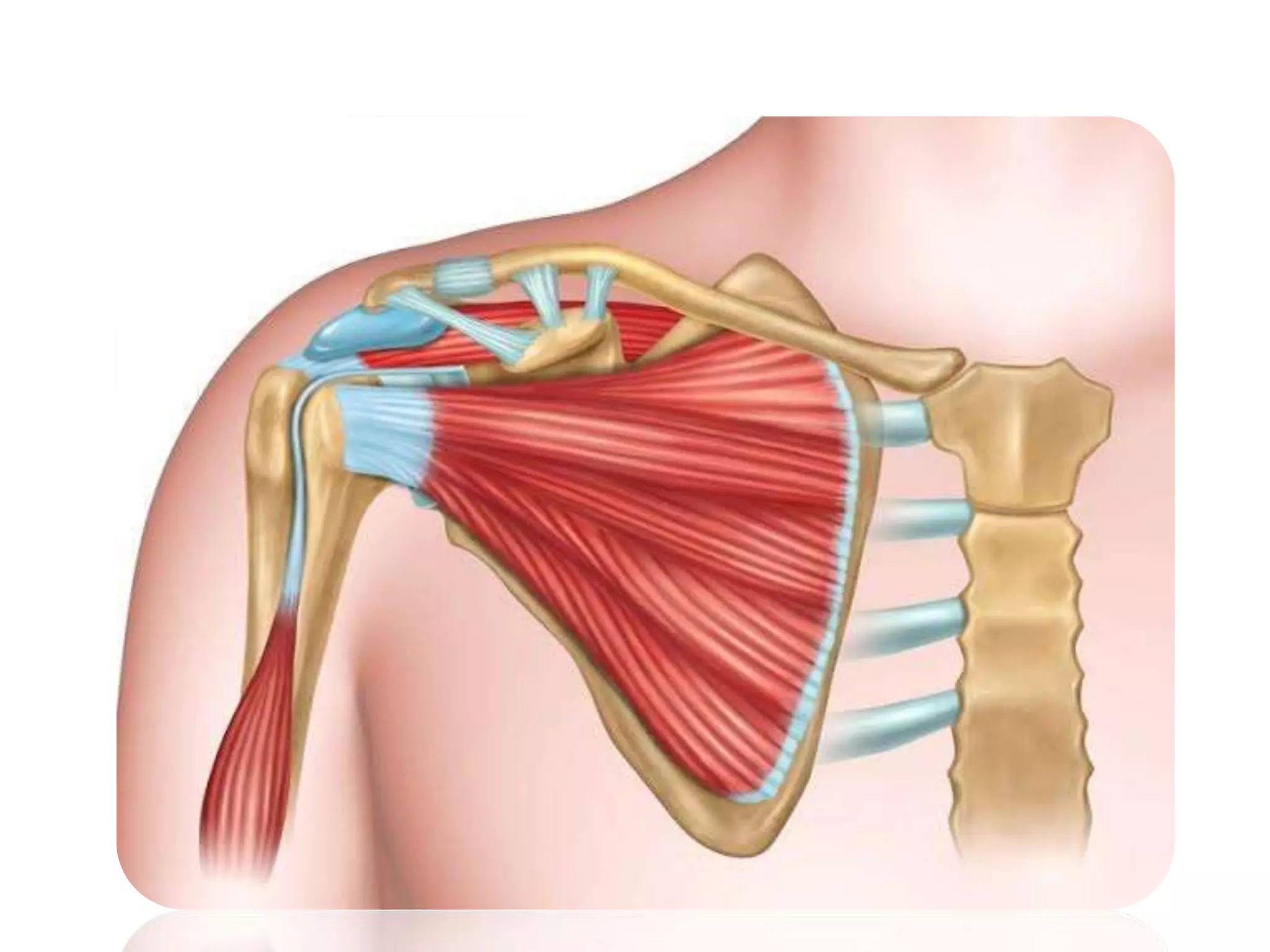








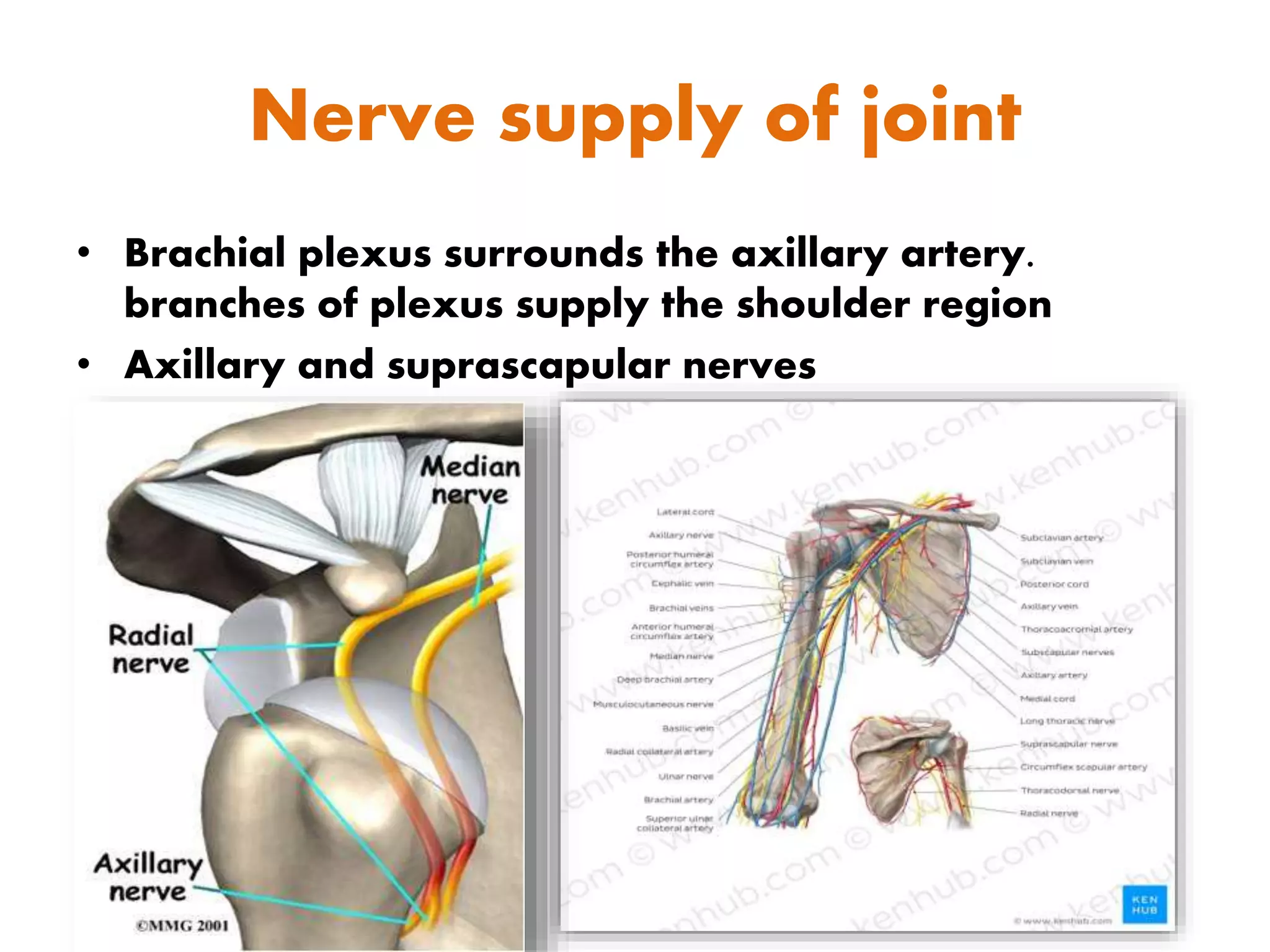
























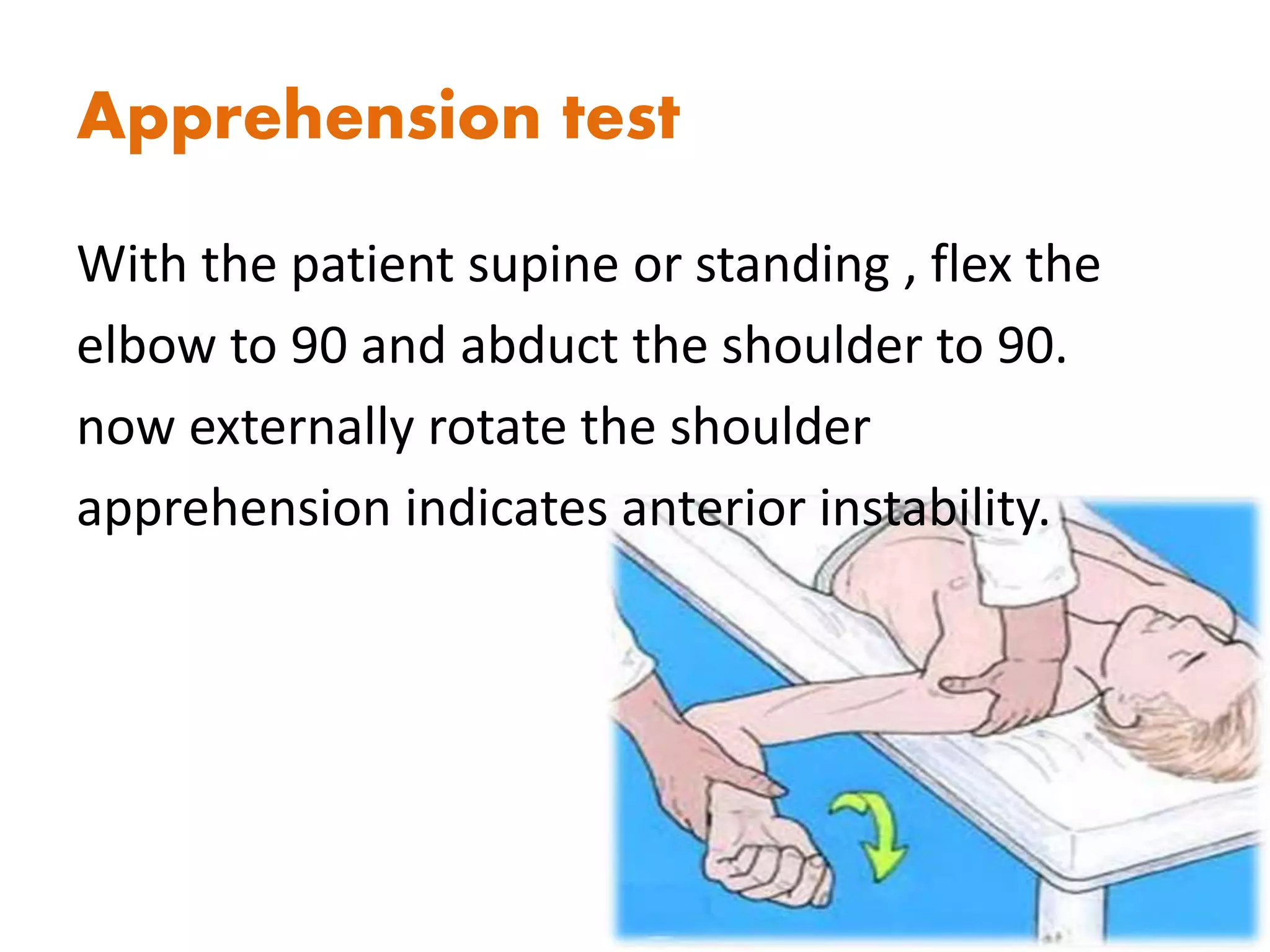





This document provides an overview of the anatomy, articulations, ligaments, muscles, blood supply, and examination of the shoulder joint. It discusses the key bones (clavicle, scapula, humerus), joints (glenohumeral, acromioclavicular), ligaments (glenohumeral, coracohumeral), muscles (rotator cuff, deltoid), and nerves (brachial plexus, axillary, suprascapular) involved. It outlines the process for examining a patient with shoulder pain, including inspection, palpation, active and passive range of motion testing, and special tests (e.g. impingement tests, apprehen















































![Shoulder_joint_and_applied_aspects[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/shoulderjointandappliedaspects1-240425164911-e75cbd49-thumbnail.jpg?width=640&height=640&fit=bounds)



















