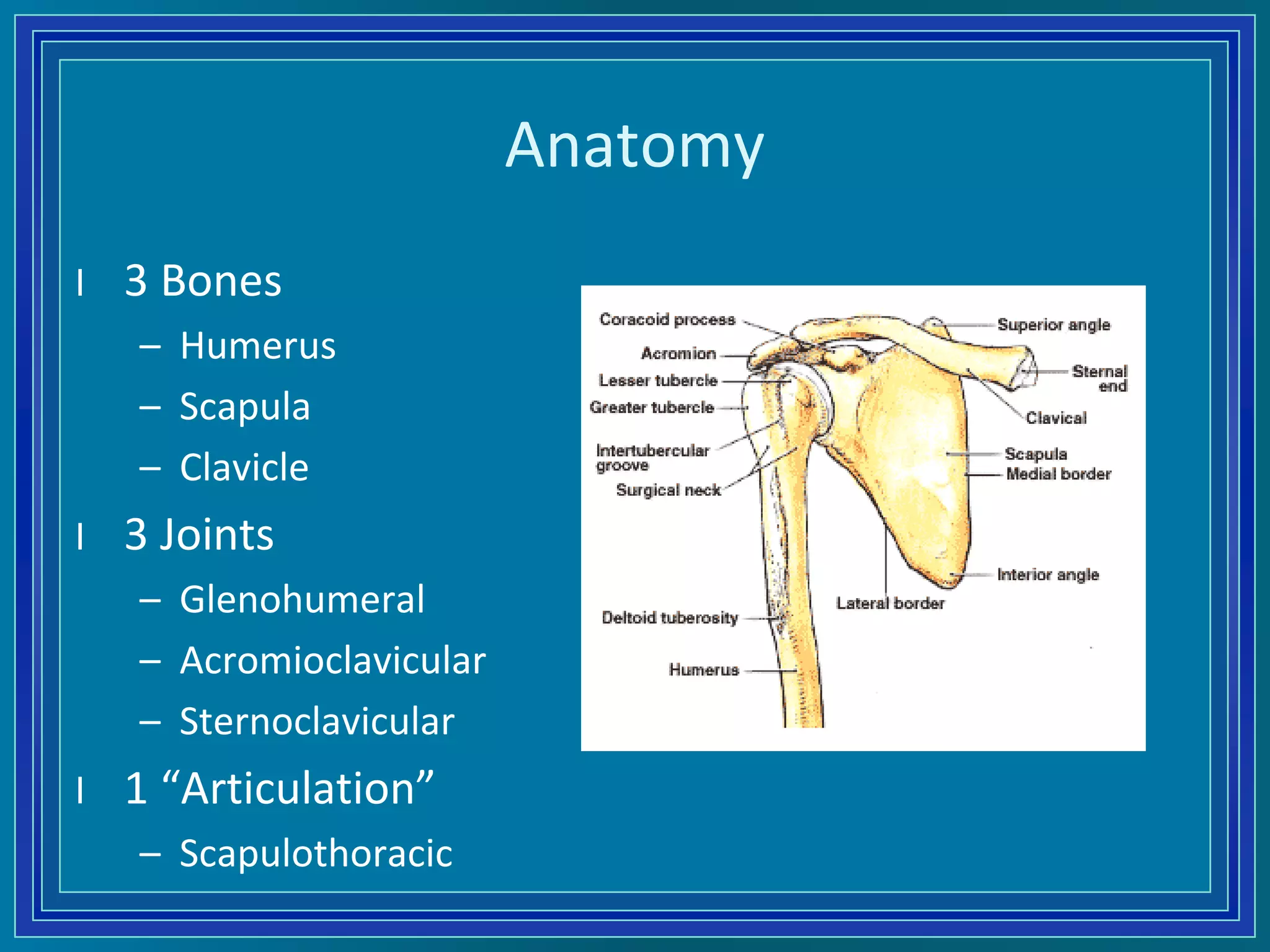
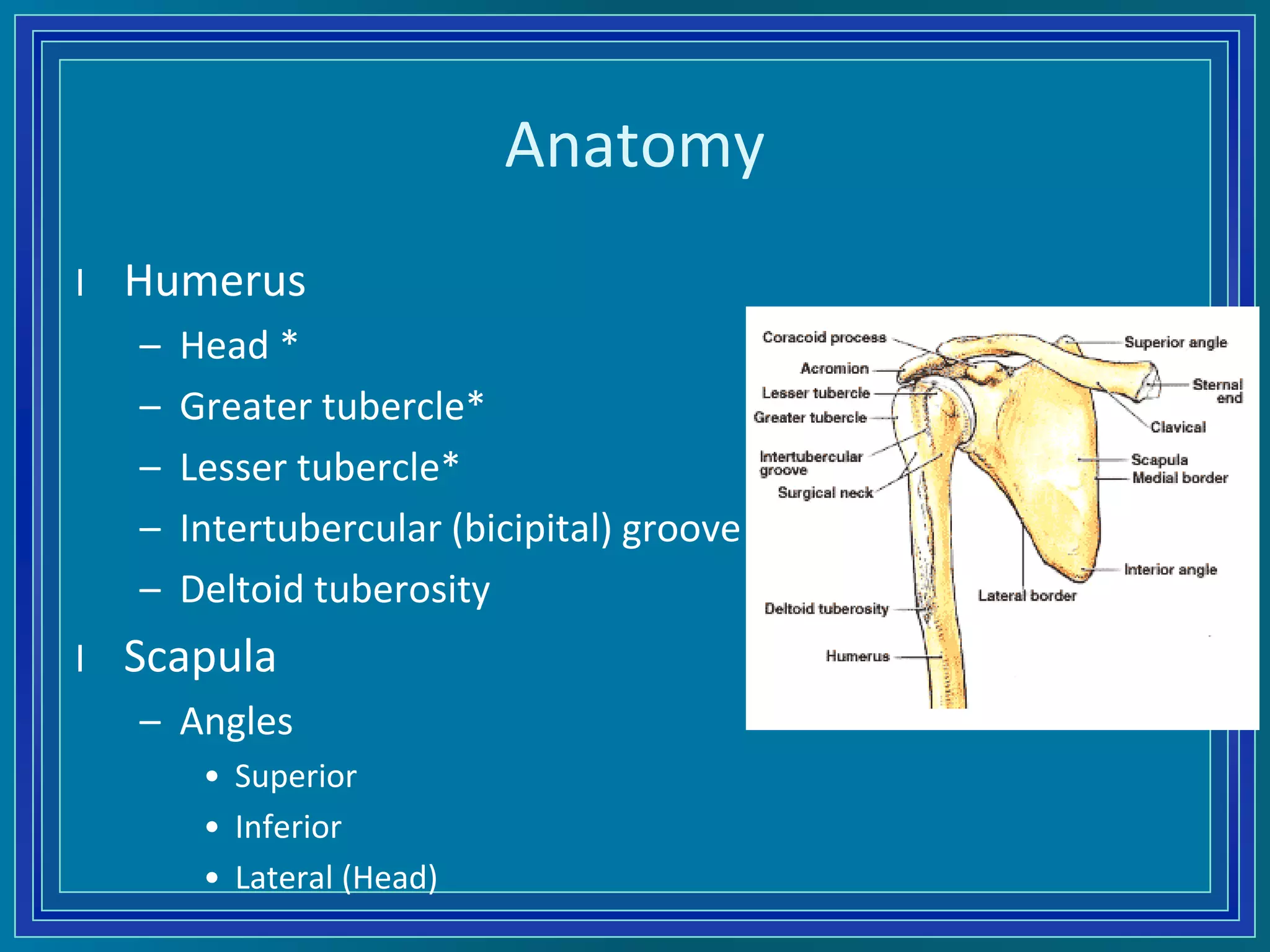
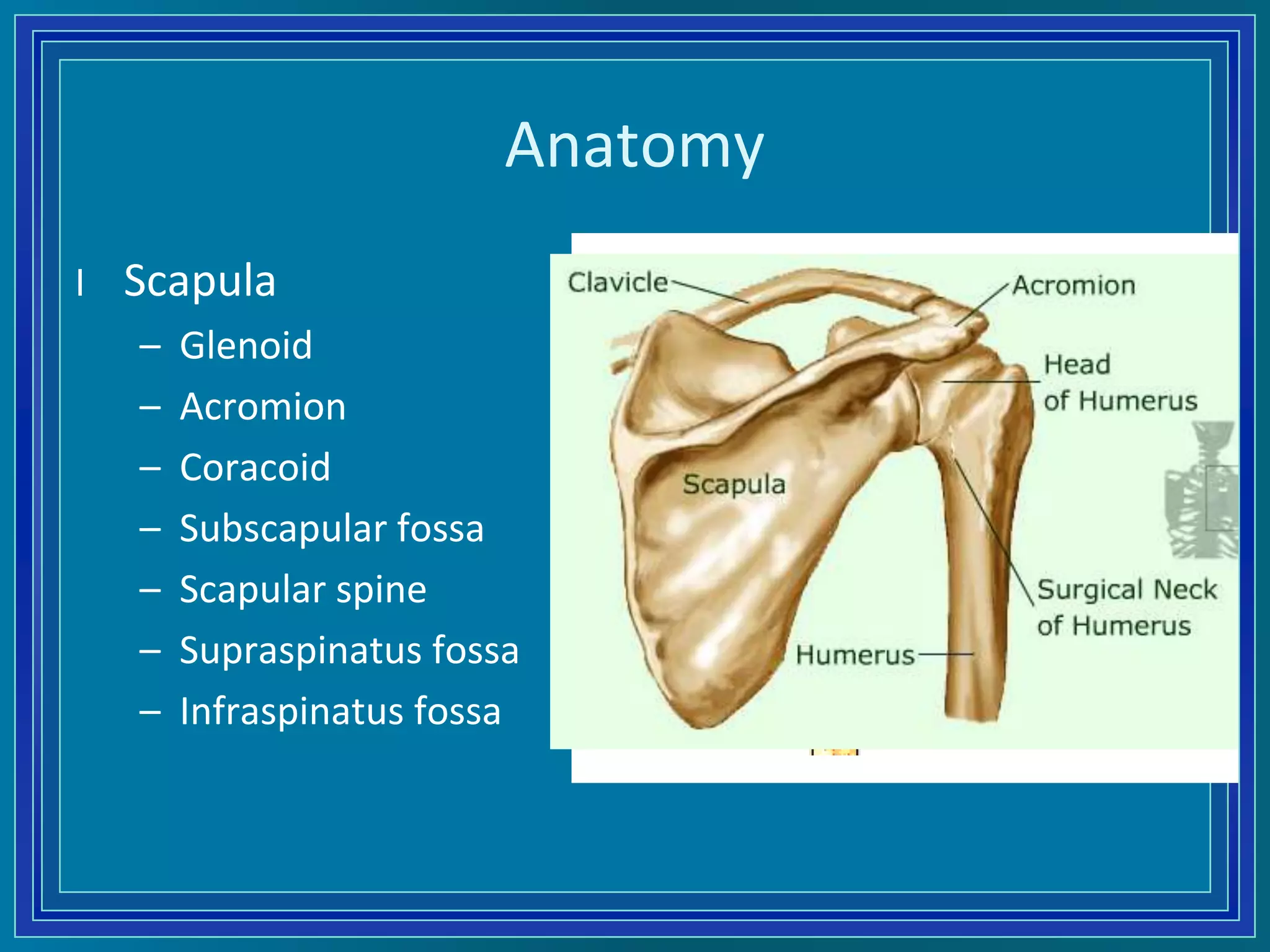
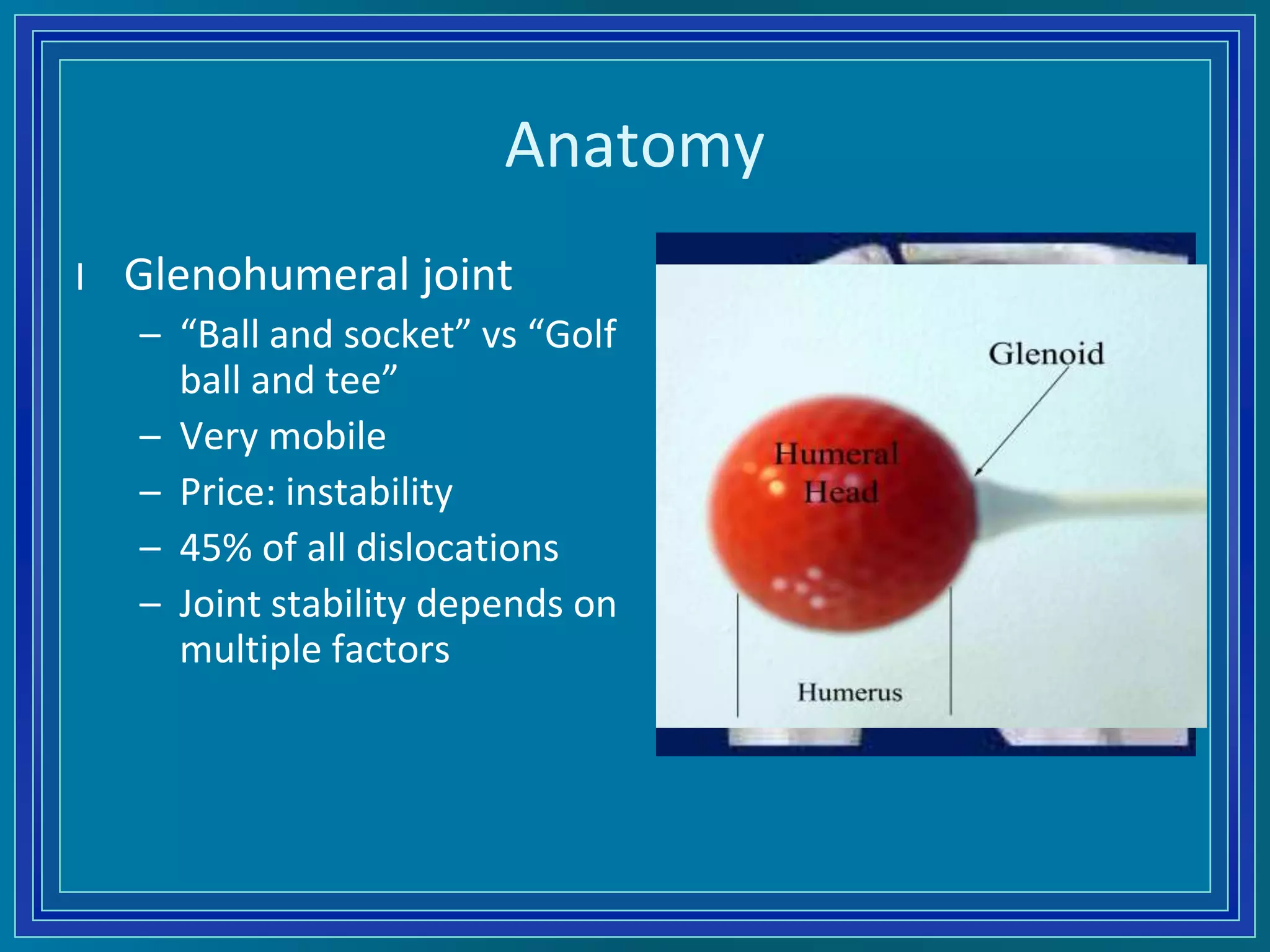
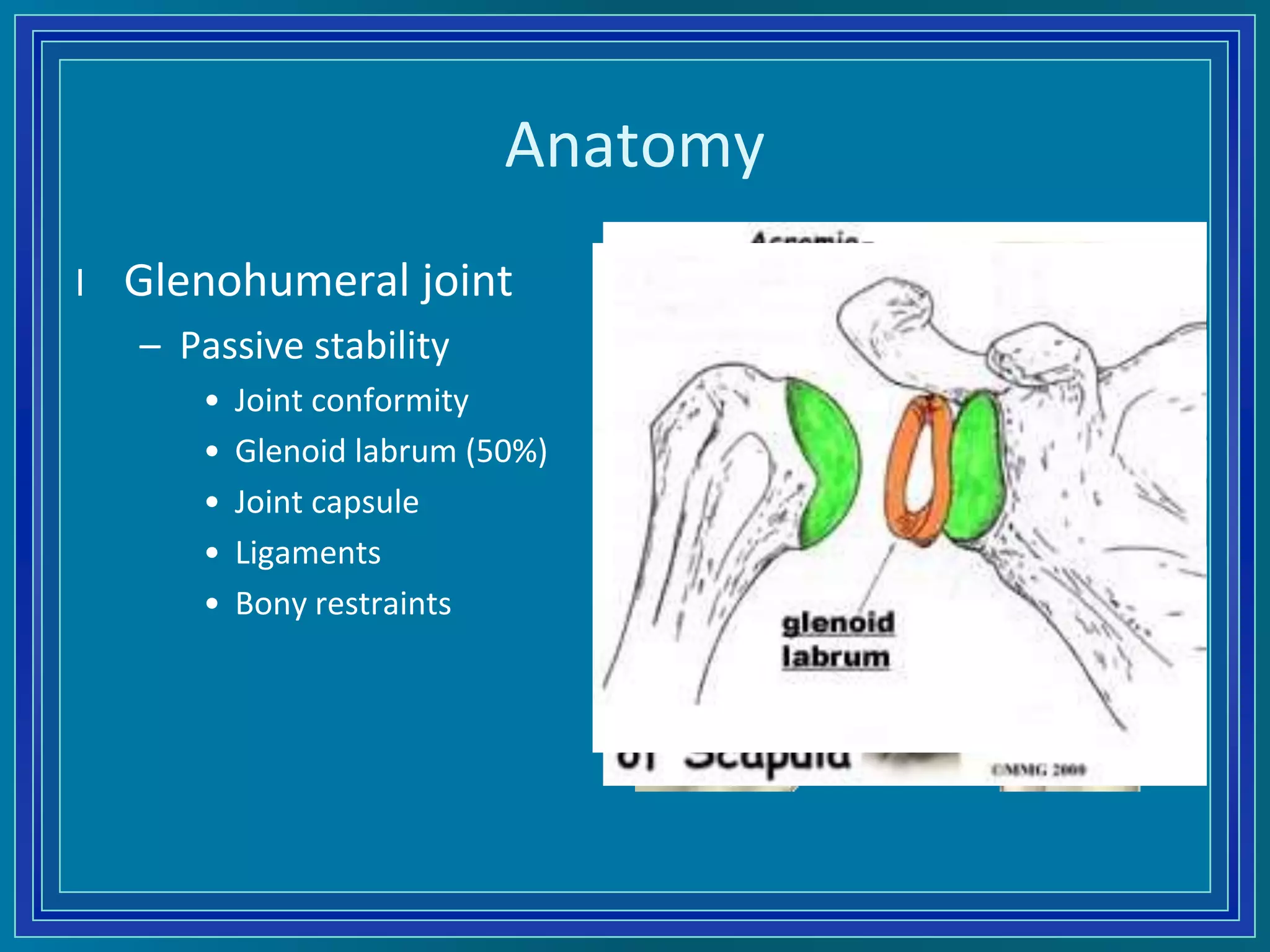
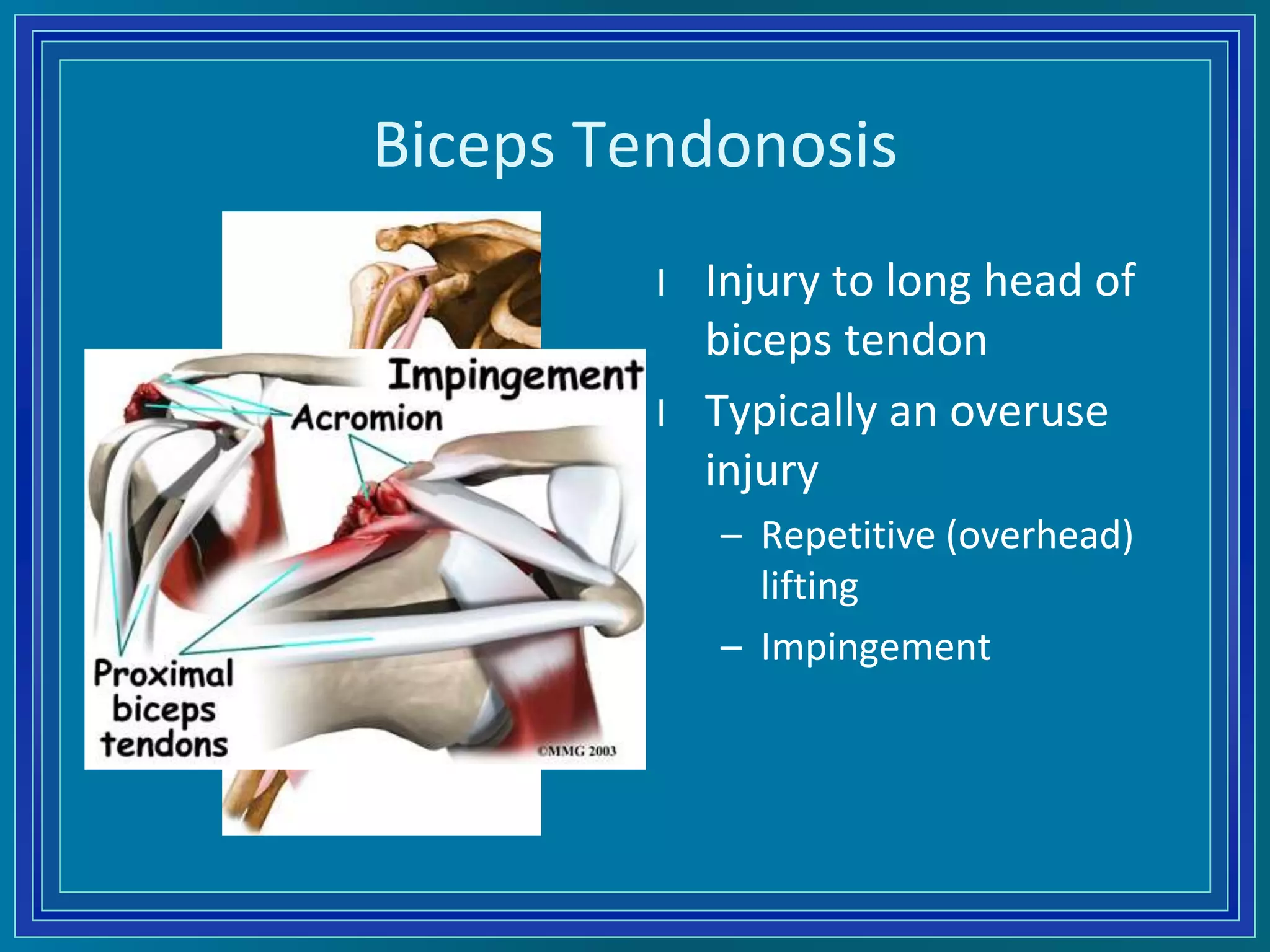
This document provides an overview of the anatomy, differential diagnosis, clinical history, and physical examination of the shoulder. It reviews the pertinent bones, joints, muscles, nerves and bursae of the shoulder. Common shoulder injuries are discussed such as impingement syndrome, rotator cuff tears, biceps tendonitis, AC joint injuries, instability and labral tears. The physical exam section describes techniques for inspection, palpation, range of motion testing, strength testing and special tests used to evaluate the shoulder.