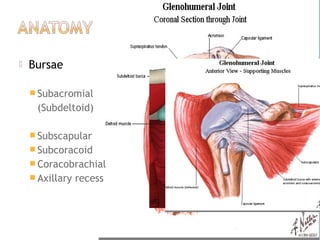
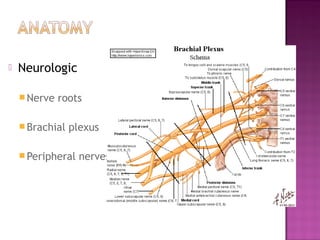
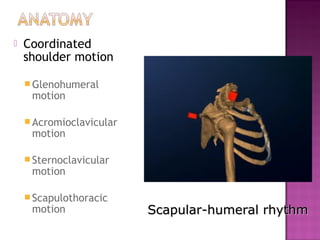
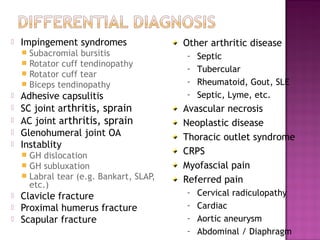
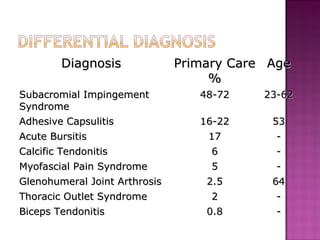
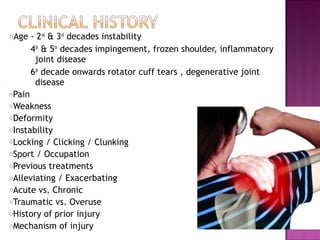
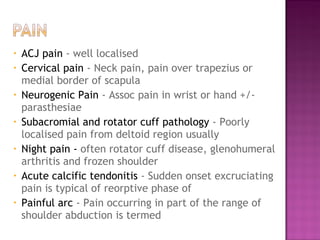

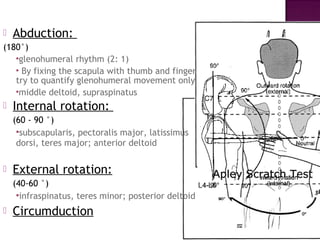
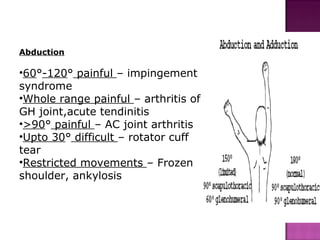

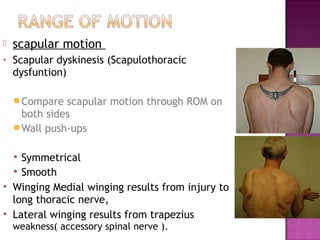
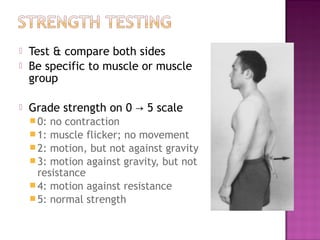






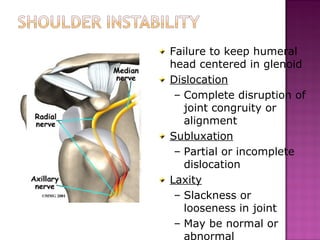
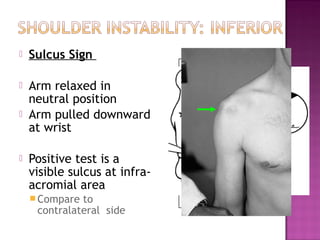

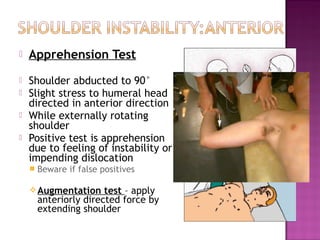
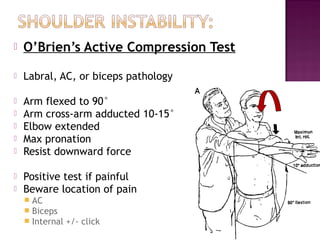
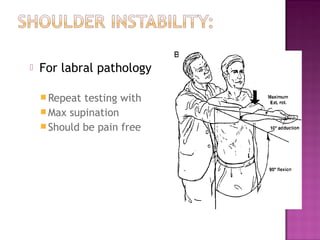
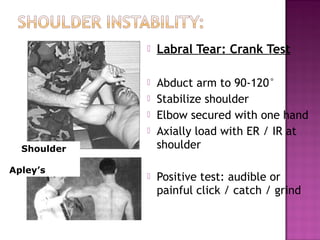
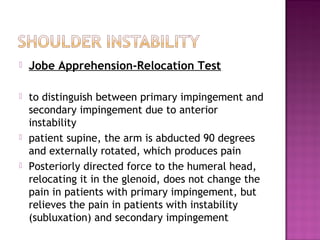



This document provides an extensive overview of shoulder anatomy, common injuries, and associated conditions, focusing on the glenohumeral joint and its mechanics. It discusses differential diagnoses, clinical history, and physical examination techniques relevant to shoulder pain, as well as specific tests and symptoms related to various shoulder pathologies. A thorough understanding of the musculature, joint stability, and motion are emphasized to aid in diagnosis and treatment planning.