Downloaded 89 times

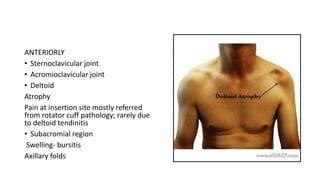
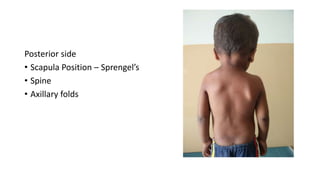
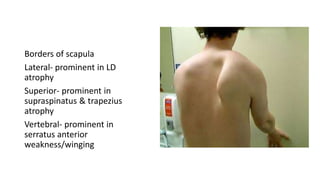
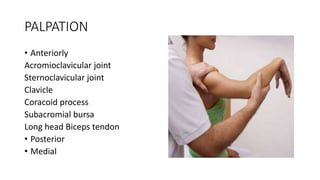
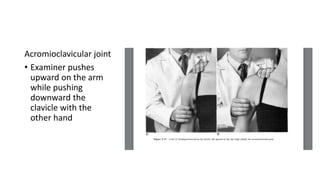
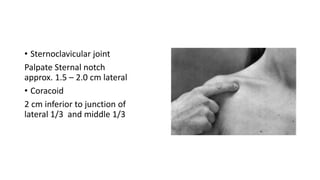

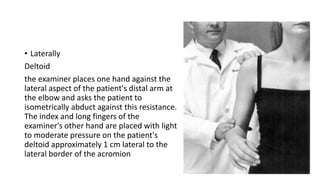

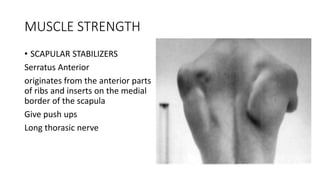
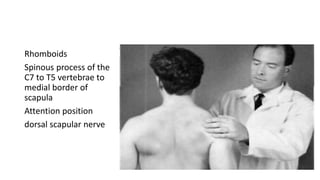

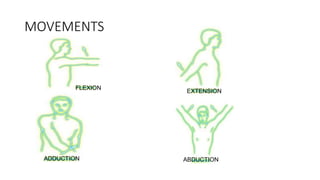
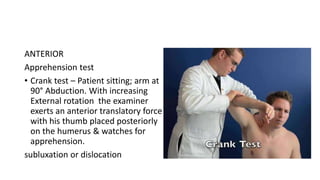
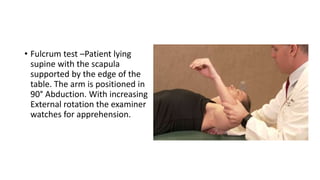
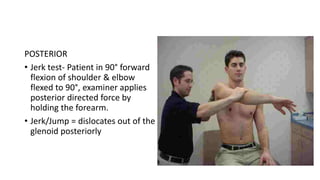

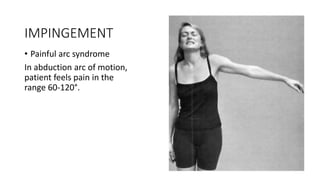






The document summarizes the steps for examining the shoulder, including: Inspection of the anterior, posterior, and lateral sides. Palpation of structures like the acromioclavicular joint, coracoid process, and long head of the biceps tendon. Assessment of muscle strength for scapular stabilizers. Evaluation of shoulder movements and special tests for conditions like instability, impingement, rotator cuff tears, and more. The examination provides a thorough overview of evaluating the structures and function of the shoulder.























































































