Downloaded 197 times
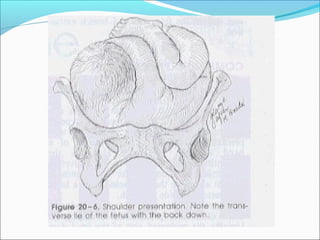
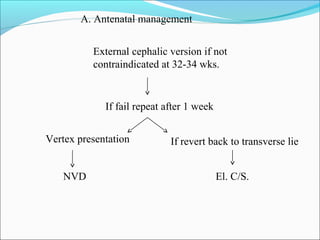
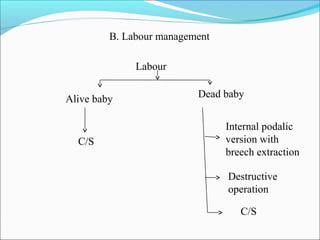
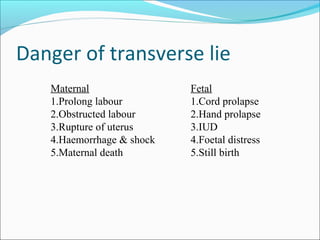
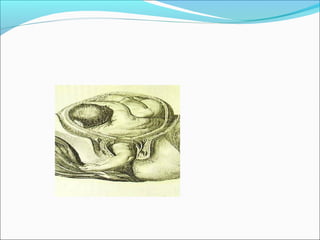


This document discusses shoulder presentation during childbirth. Some key points: - Shoulder presentation occurs when the fetus is transverse instead of longitudinal in the birth canal, with the shoulder as the presenting part. It has an incidence of 0.3%. - Diagnosis is made through inspection of asymmetric uterine enlargement, palpation finding the fetal back on one side and breech on the other, and ultrasound confirming the transverse lie. - Management involves attempting external cephalic version to convert to a vertex presentation if possible. If that fails or labor begins, cesarean section is usually required due to the risks of obstructed labor and fetal distress.























































































