Downloaded 30 times
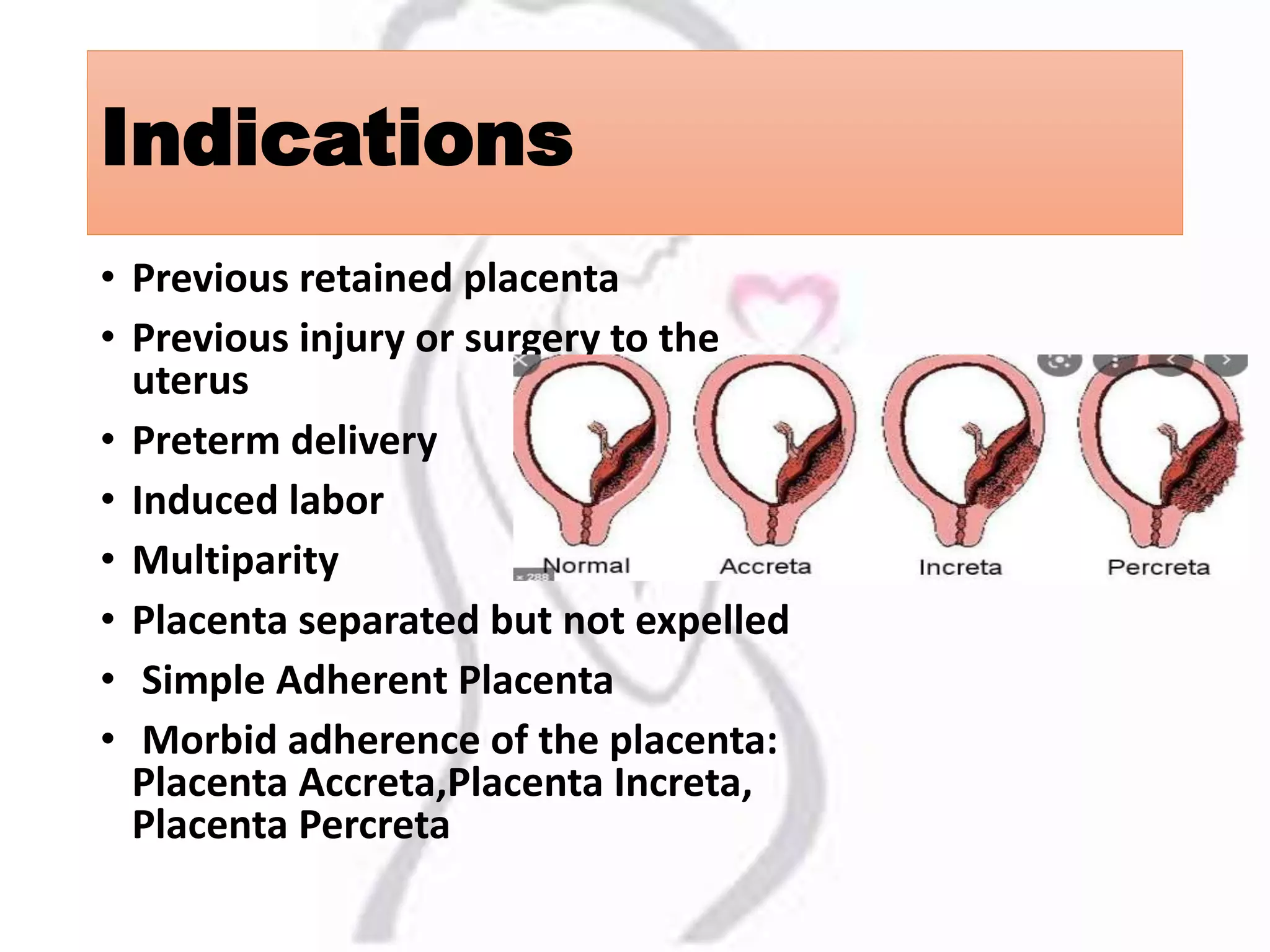
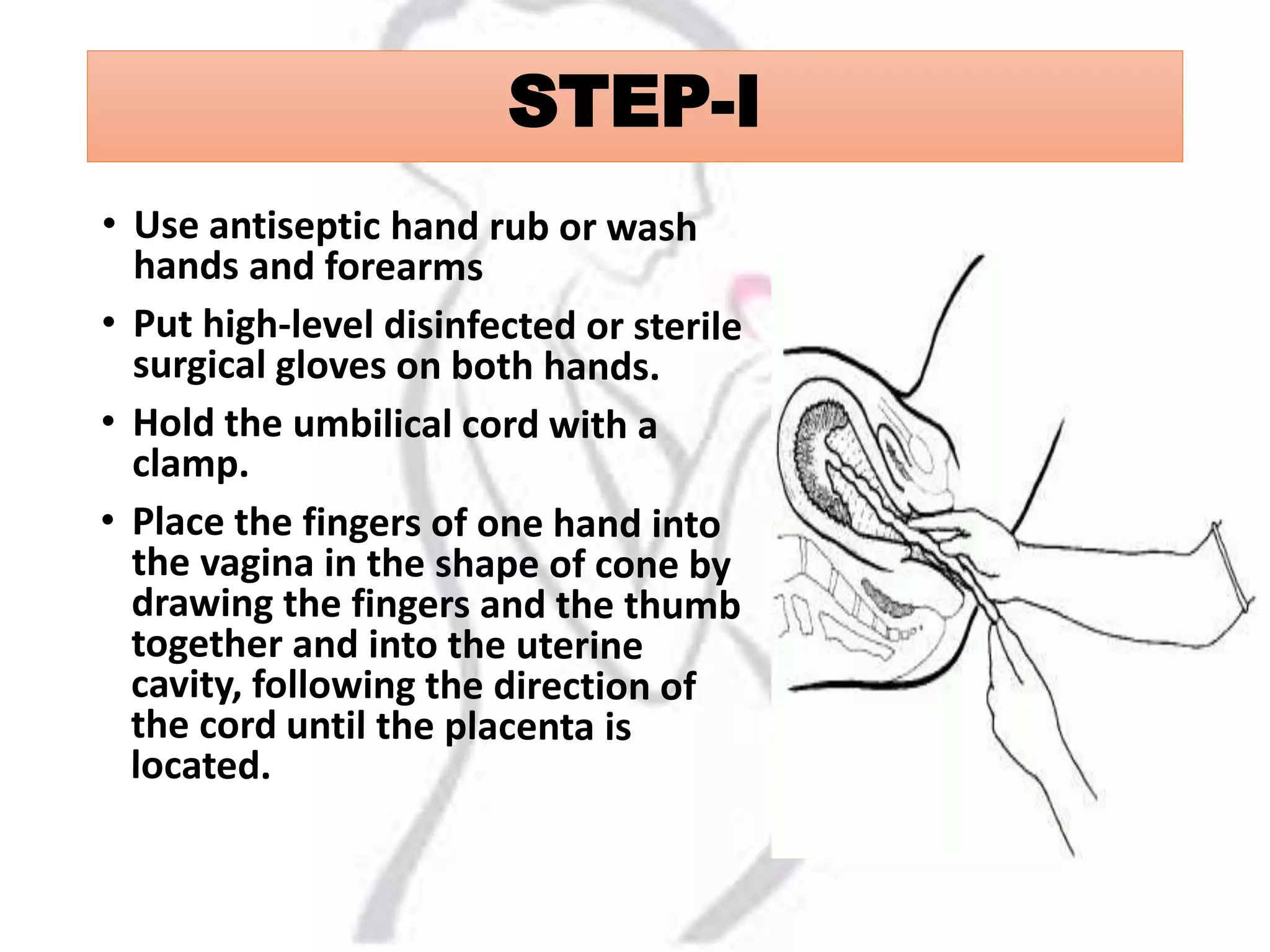
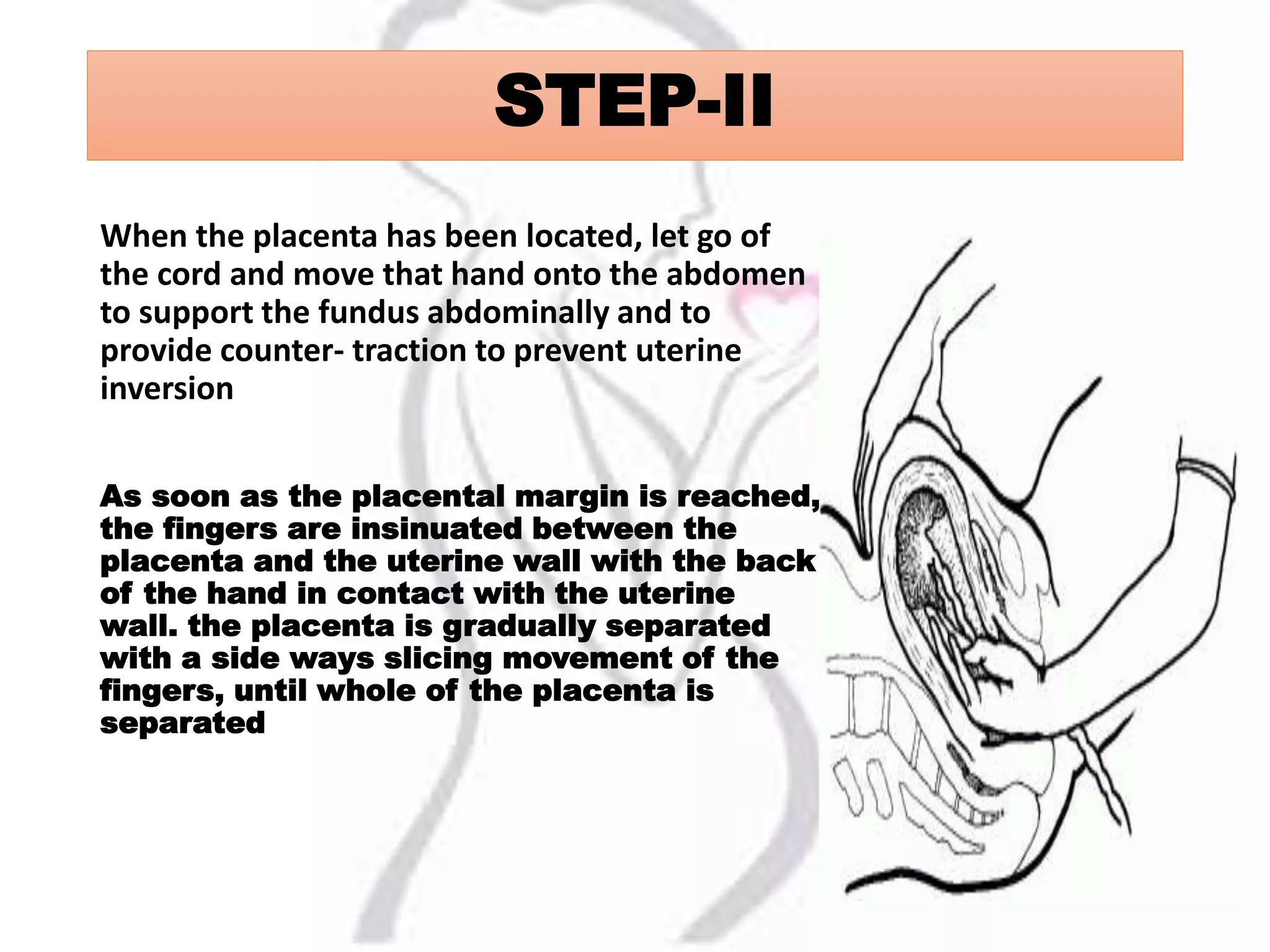
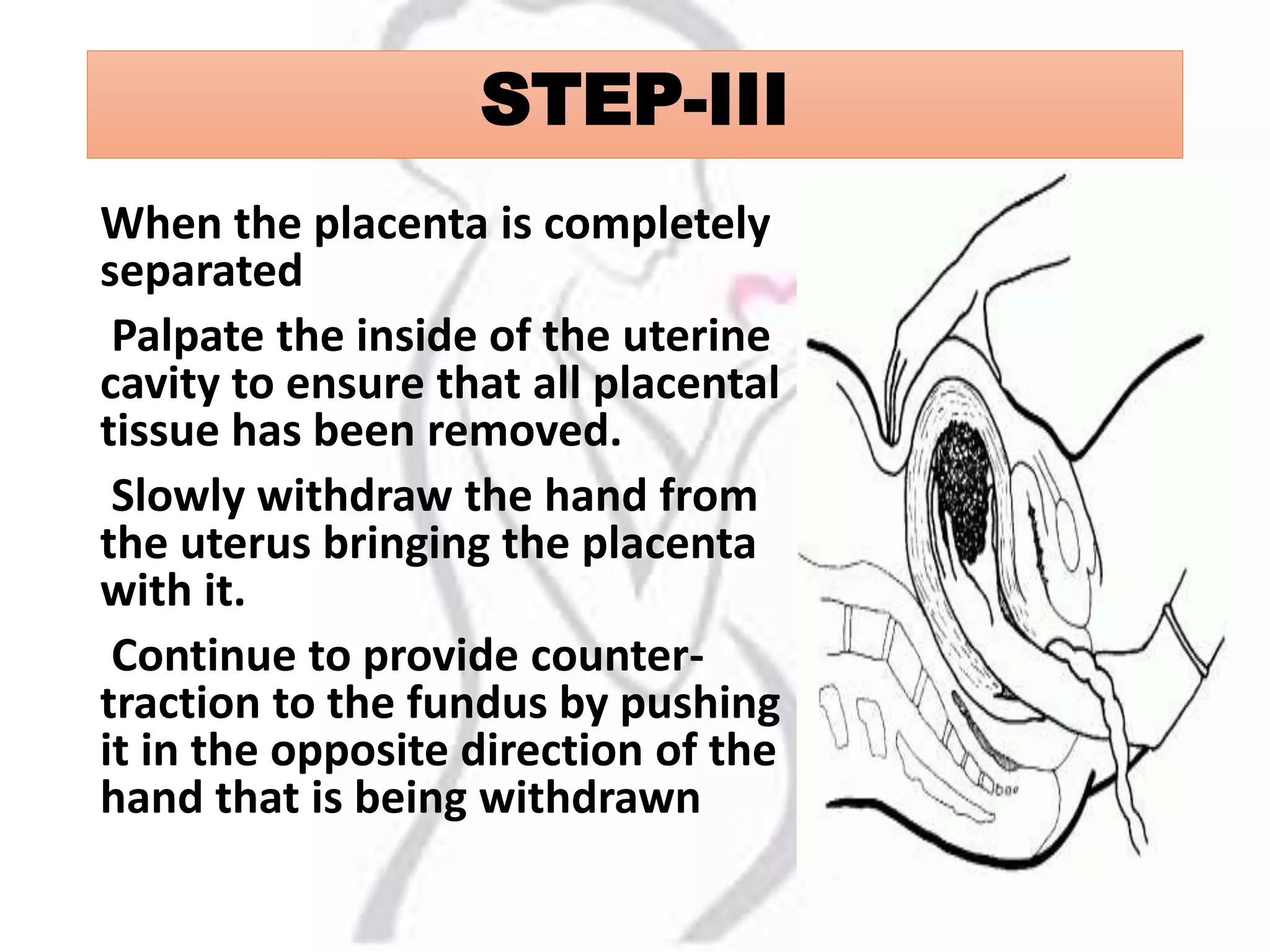


Manual removal of the placenta is conducted when the placenta remains in the uterus beyond 30 minutes after childbirth. The procedure involves various steps including the administration of anesthesia, careful separation of the placenta, and post-procedural monitoring for complications. Indications for this procedure include previous retained placenta, uterine surgery, and certain complications related to placenta adherence.

















































































