This document discusses transverse lie and cord prolapse during labor. It provides information on:
1) The definition and causes of transverse lie, where the fetus lies horizontally across the uterus with the shoulder over the pelvic inlet.
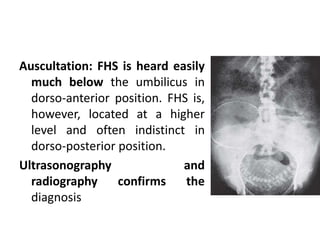
2) The diagnosis of transverse lie which involves abdominal and vaginal examinations to identify fetal parts and position. Ultrasound can also confirm the diagnosis.
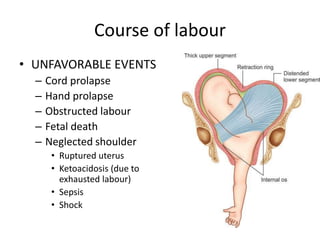
3) The risks of transverse lie including cord prolapse, obstructed labor, and fetal death. Management involves external cephalic version or cesarean section.
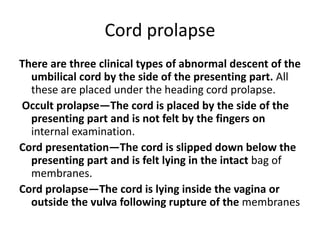
4) The definition, causes, diagnosis, and management of cord prolapse, which requires immediate delivery by cesarean section if the fetus is alive or




















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)





![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)











