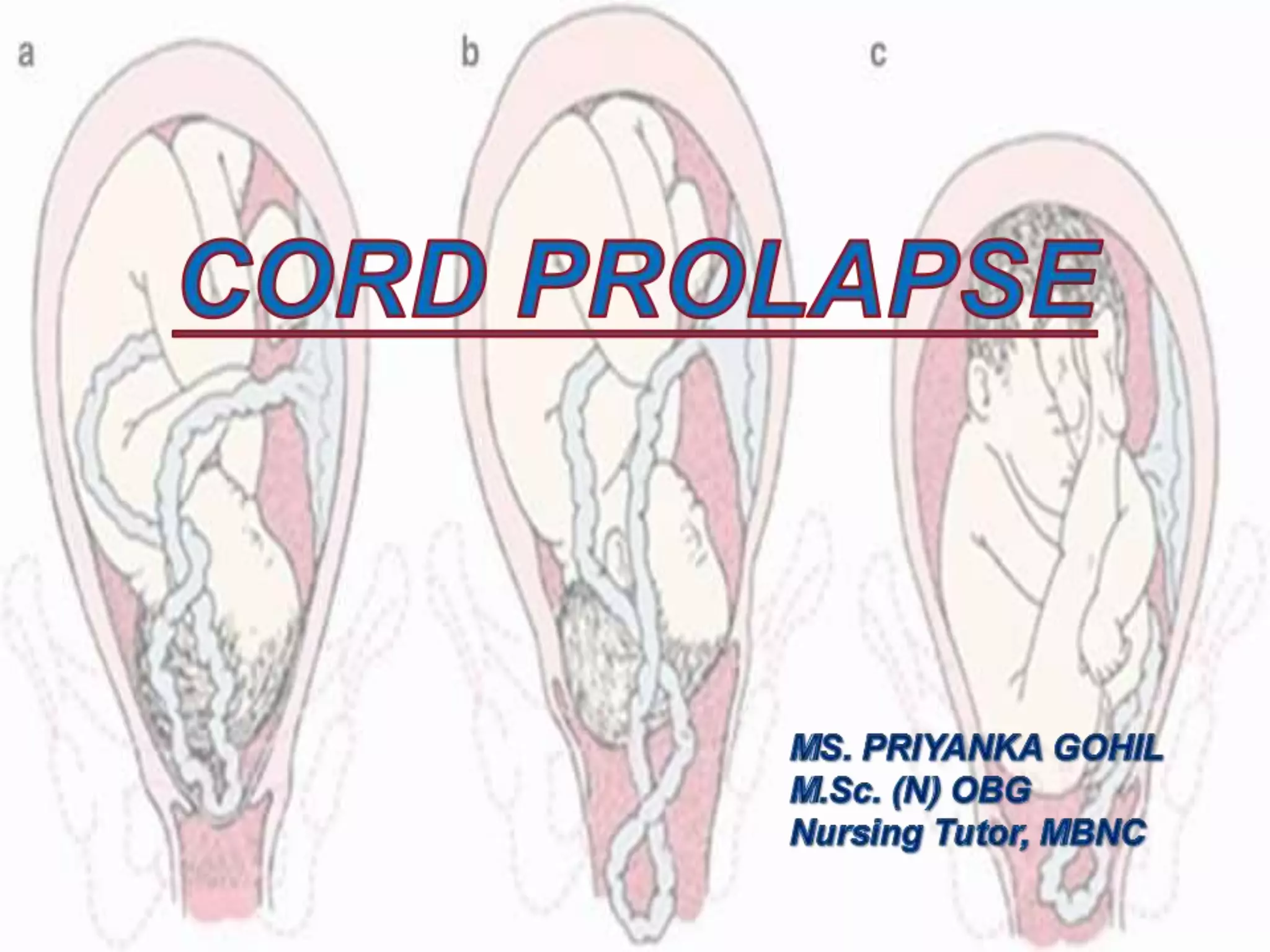
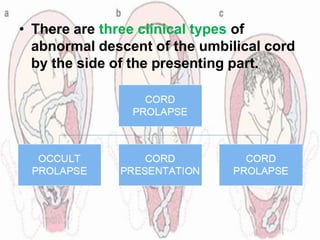
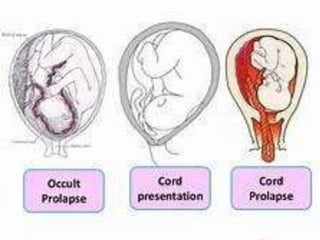
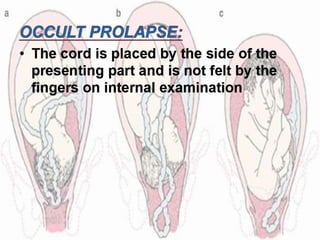
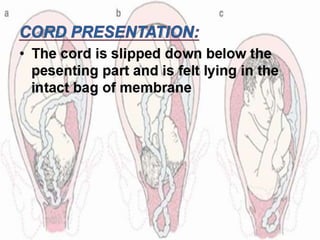
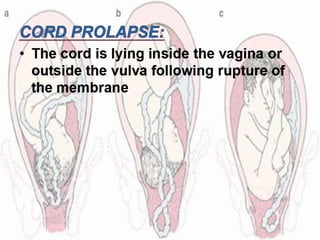
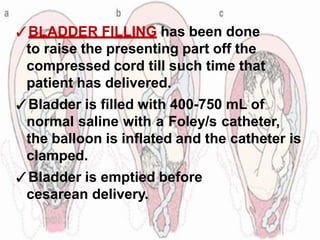
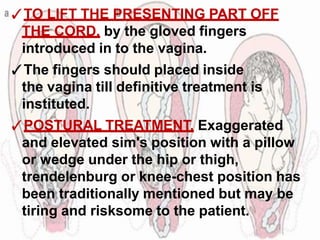
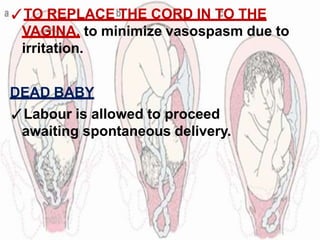
This document discusses umbilical cord prolapse during delivery, including risk factors, diagnosis, and management approaches. It notes that cord prolapse occurs in 1 in 3,000 deliveries and risks increase with malpresentations, contracted pelvis, prematurity, and other complications. Diagnosis involves feeling pulsation in the cord. Management depends on viability of the baby and cervical dilation, and may include cesarean delivery, forceps-assisted vaginal delivery, or temporary measures to relieve cord compression until definitive care is available. The goal is to expedite delivery to minimize risks to both baby and mother.





























































![谷歌留痕技术 [ 𝙩𝙤𝙥 𝟮𝟯𝟯. 𝙘 𝙤𝙢 ]](https://cdn.slidesharecdn.com/ss_thumbnails/top233-260130174328-3833018c-thumbnail.jpg?width=640&height=640&fit=bounds)







