Downloaded 89 times

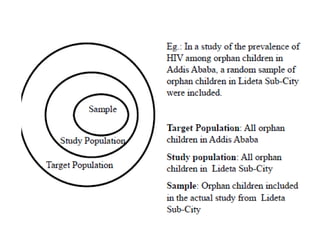




The document discusses research methodology and methods and materials sections of research proposals. It provides details on what should be included in the methods and materials section such as the study design, population, variables, data collection plan, and limitations. The methods section is important as it shows how the research will achieve its objectives and answer the research questions.











































































































