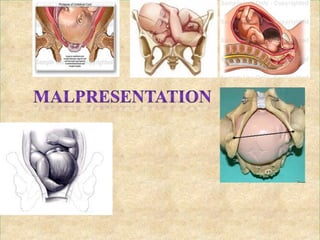
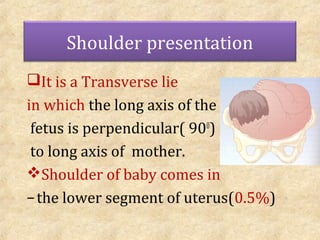
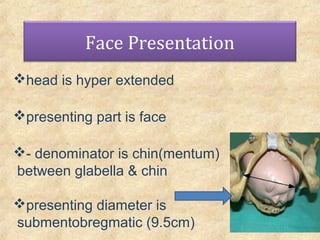
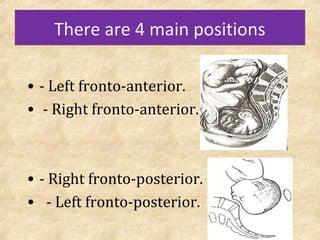
This document defines and discusses abnormal fetal positions and presentations that can occur during labor, including breech, face, brow, shoulder, transverse lie, and compound presentations. It provides the definitions, incidence rates, causes, diagnostic techniques, and management approaches for each atypical presentation. Key points covered include the different types of breech, face, brow, and shoulder positions, mechanisms of labor for each, and when external cephalic version, assisted vaginal delivery, or cesarean section are recommended.