Downloaded 134 times

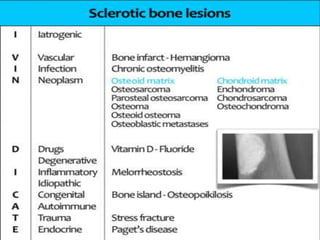












The document discusses various types of sclerotic lesions and their implications in bone pathology, emphasizing the slow-growing nature of these lesions relative to their underlying causes. It covers a range of etiologies including infections, neoplasms, drugs, and chronic conditions, along with associated imaging findings. Key differentiating factors between sclerotic lesions, benign tumors, and malignant transformations are also outlined.










































































































