Downloaded 1,022 times


























The document describes various structures of the shoulder joint that provide stability, including the labrum, biceps tendon, and glenohumeral ligaments. It discusses common labral injuries like SLAP tears and Bankart lesions caused by anterior dislocation of the humeral head. It also describes variants like Buford complex and sublabral recesses that should not be confused with pathology.
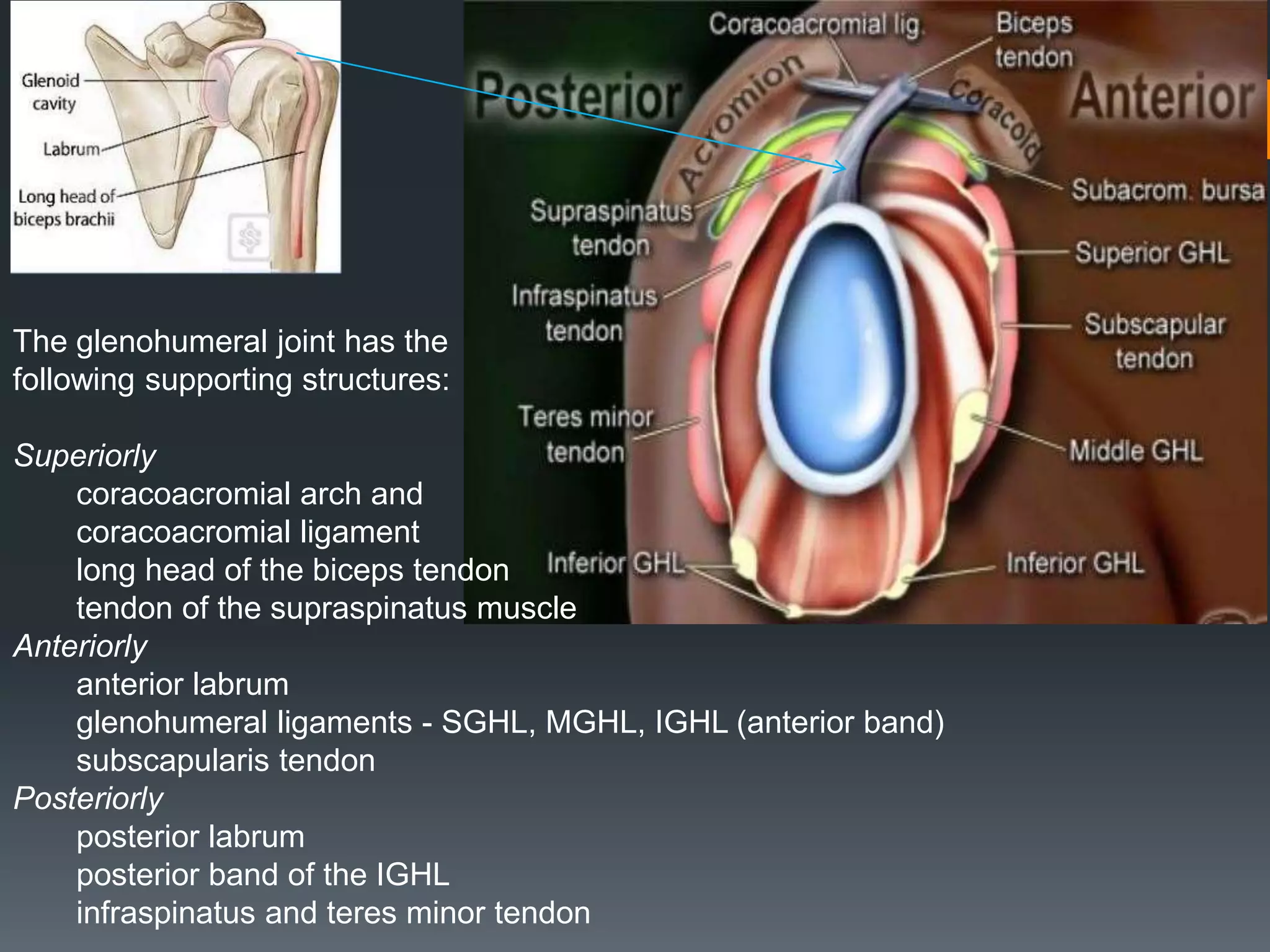
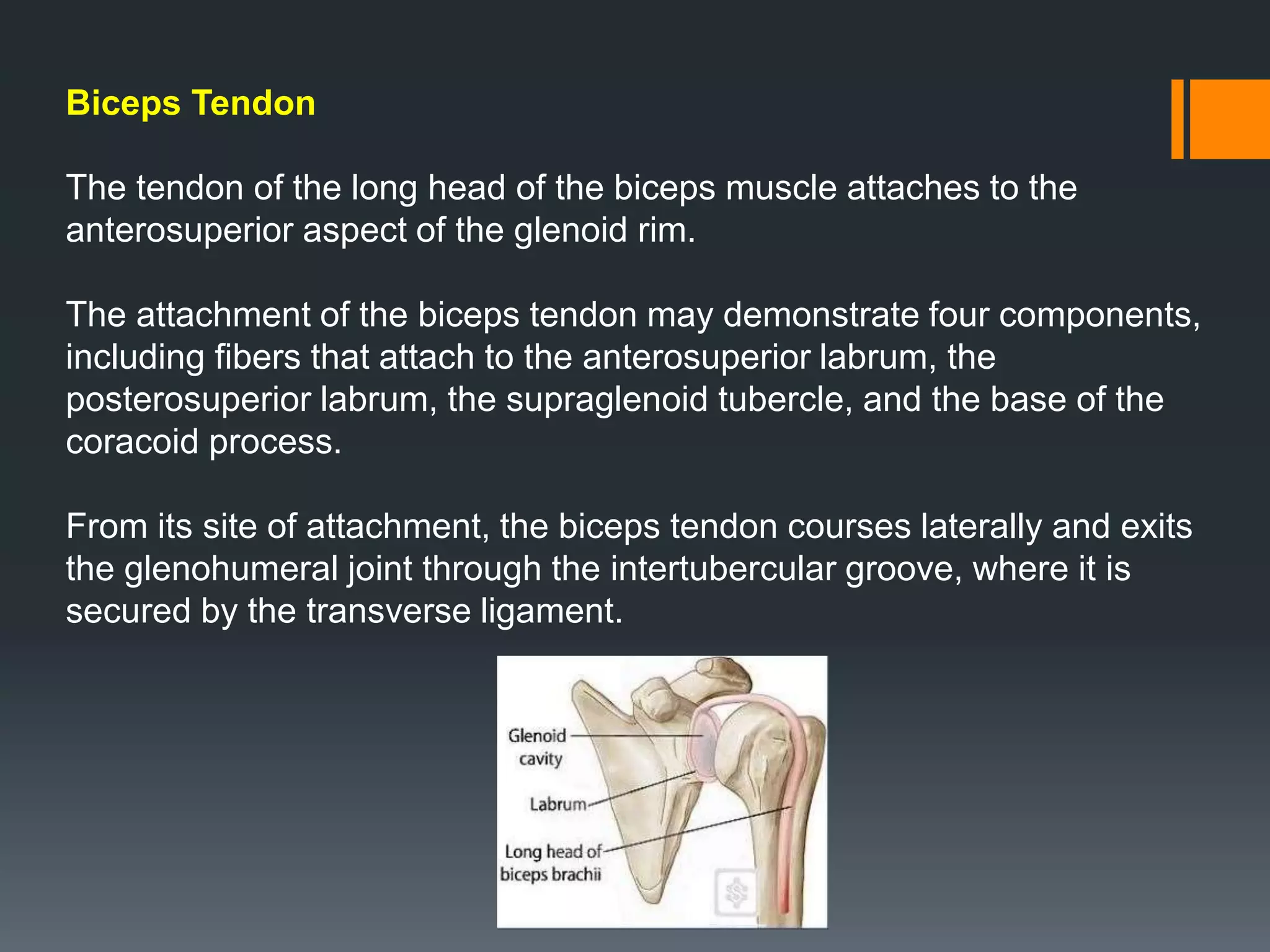
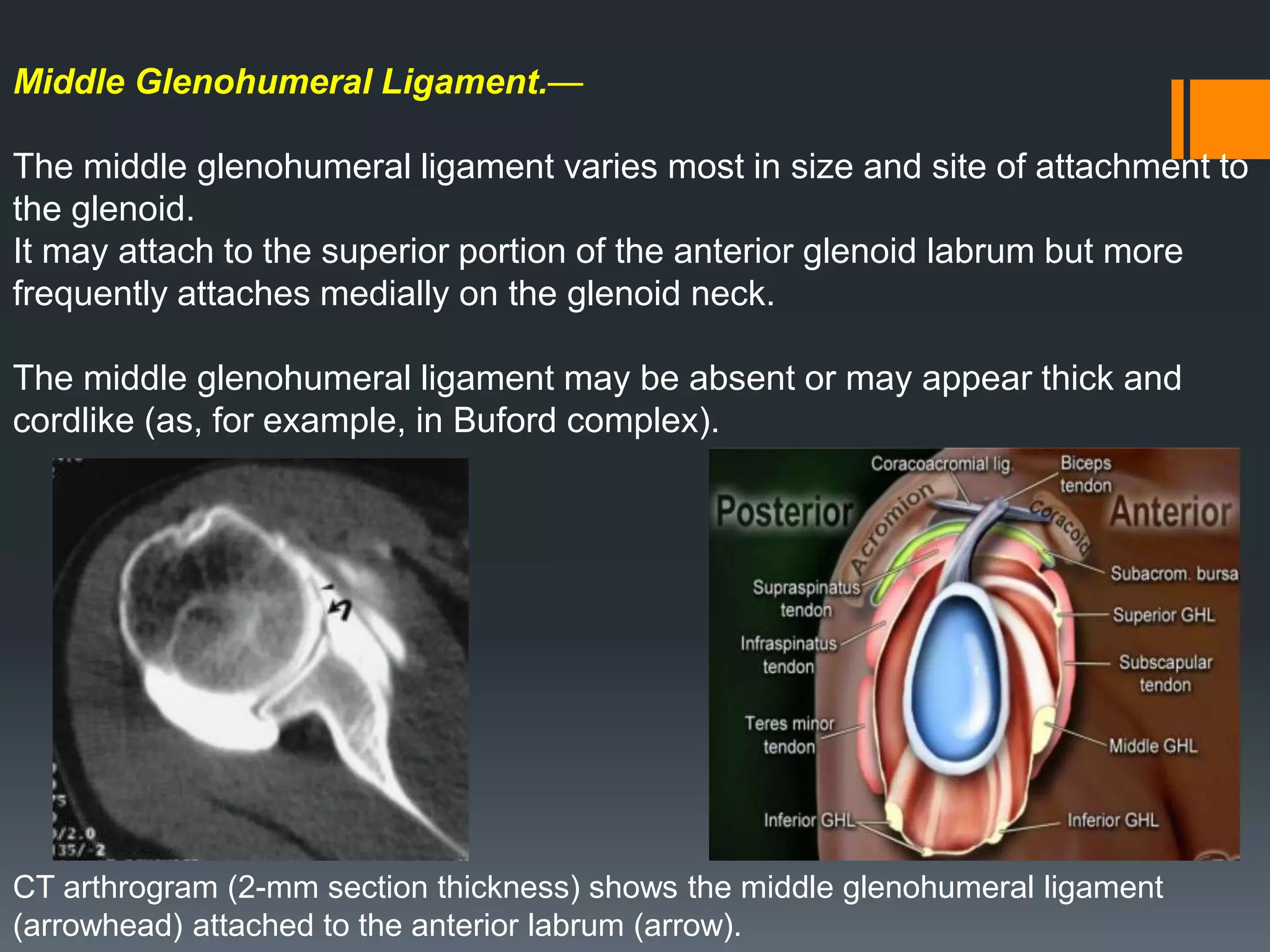
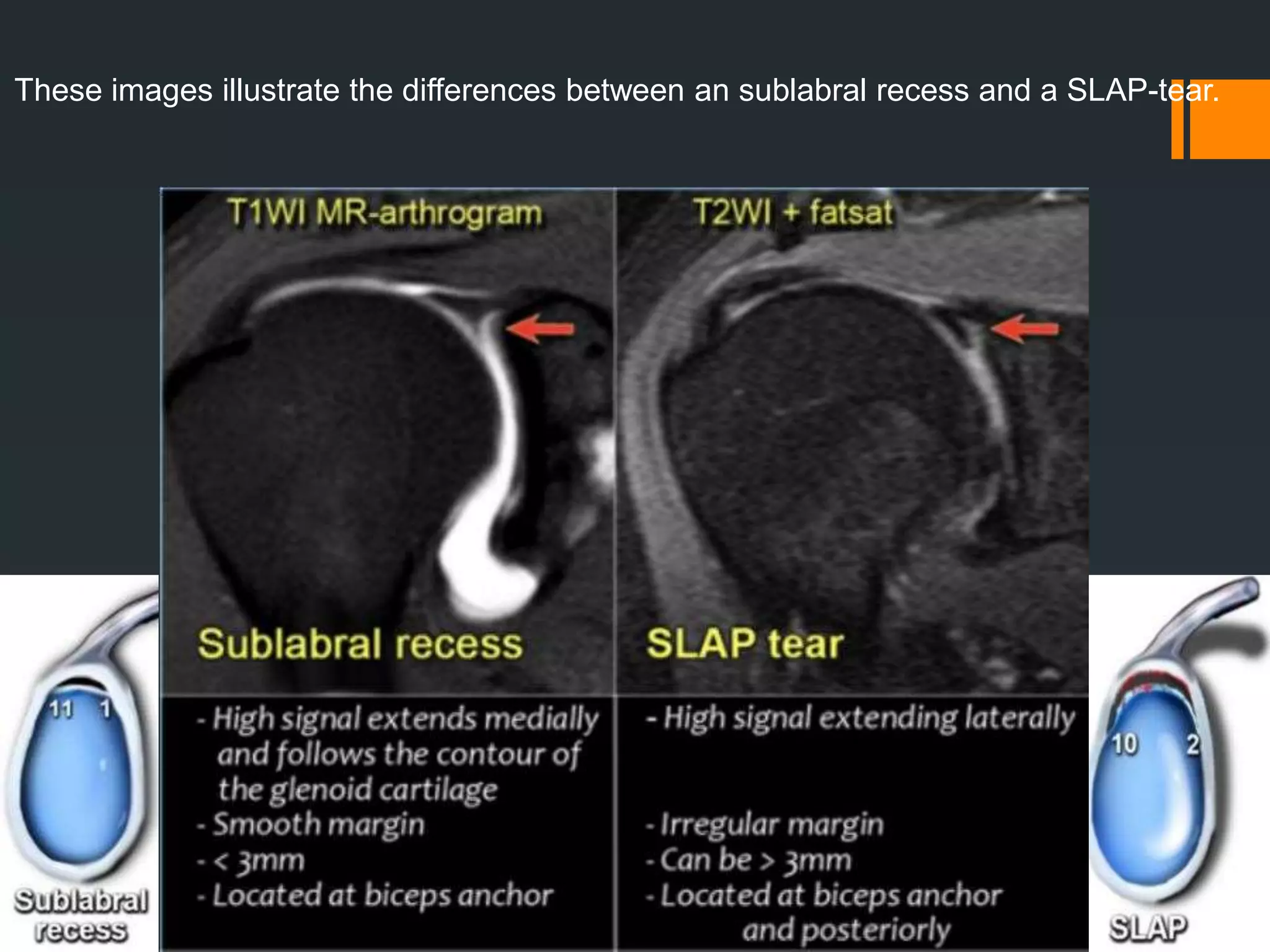
Discusses shoulder anatomy, labrum characteristics, and biceps tendon attachments, plus variants that mimic tears.
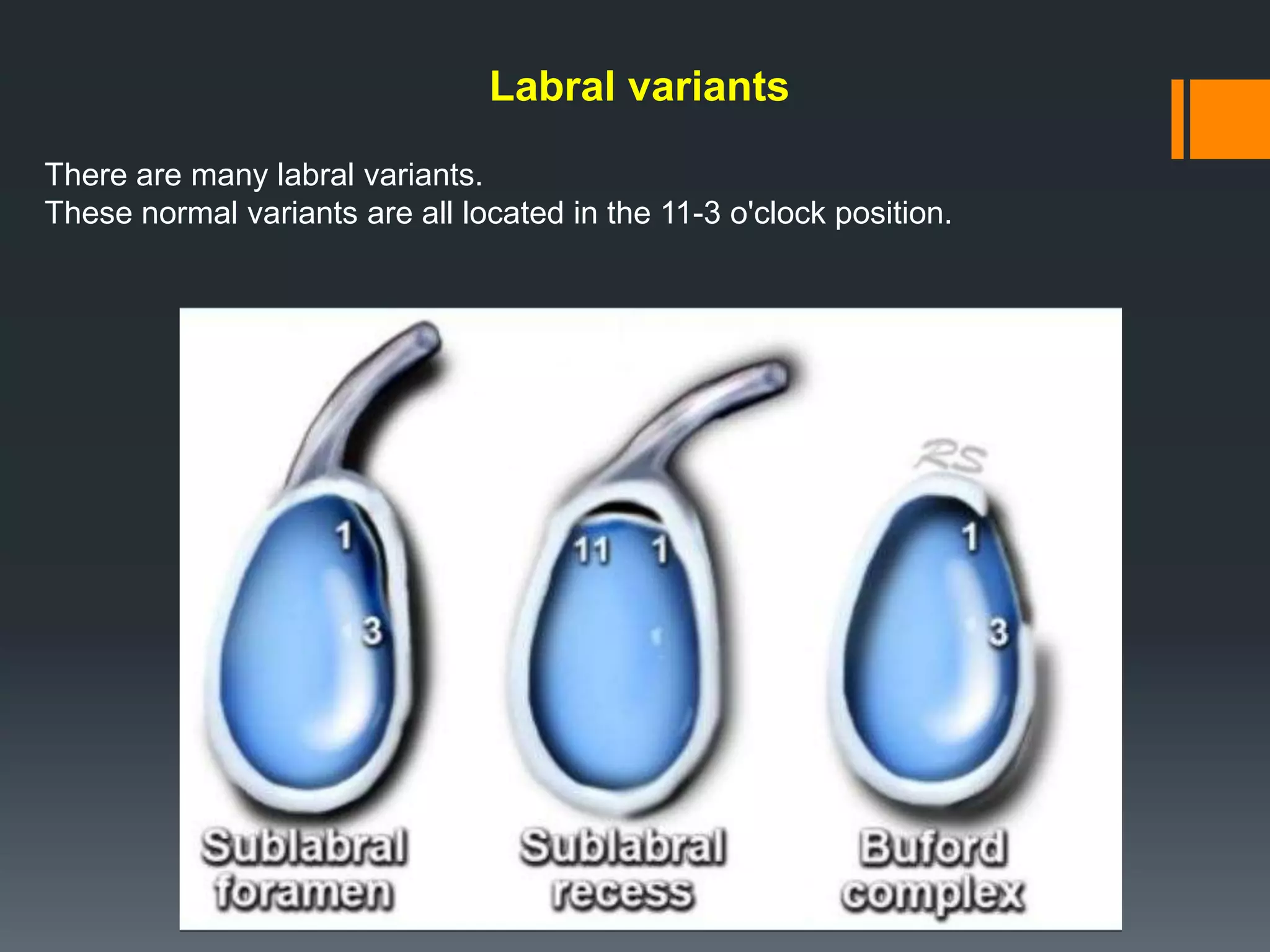
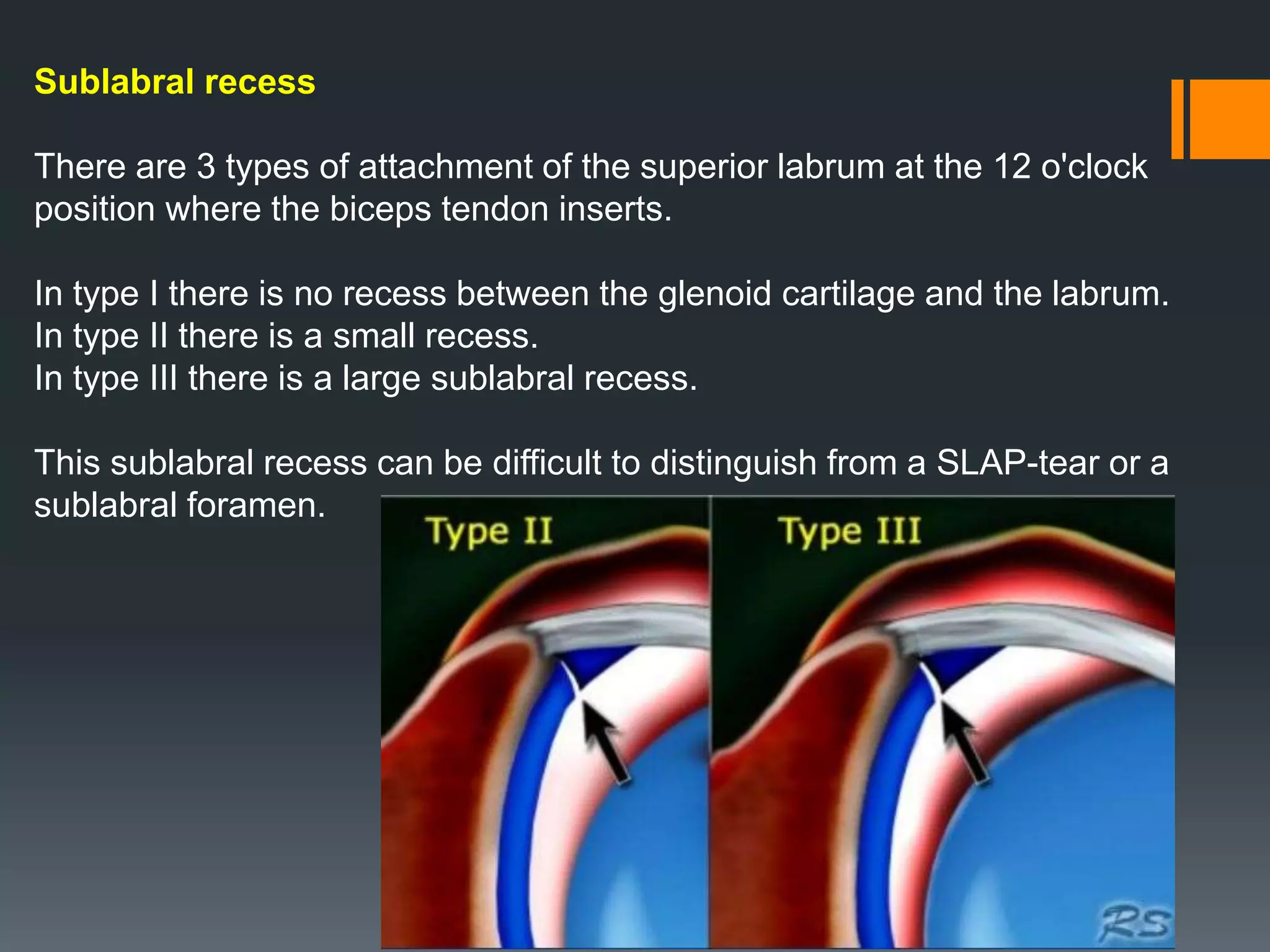
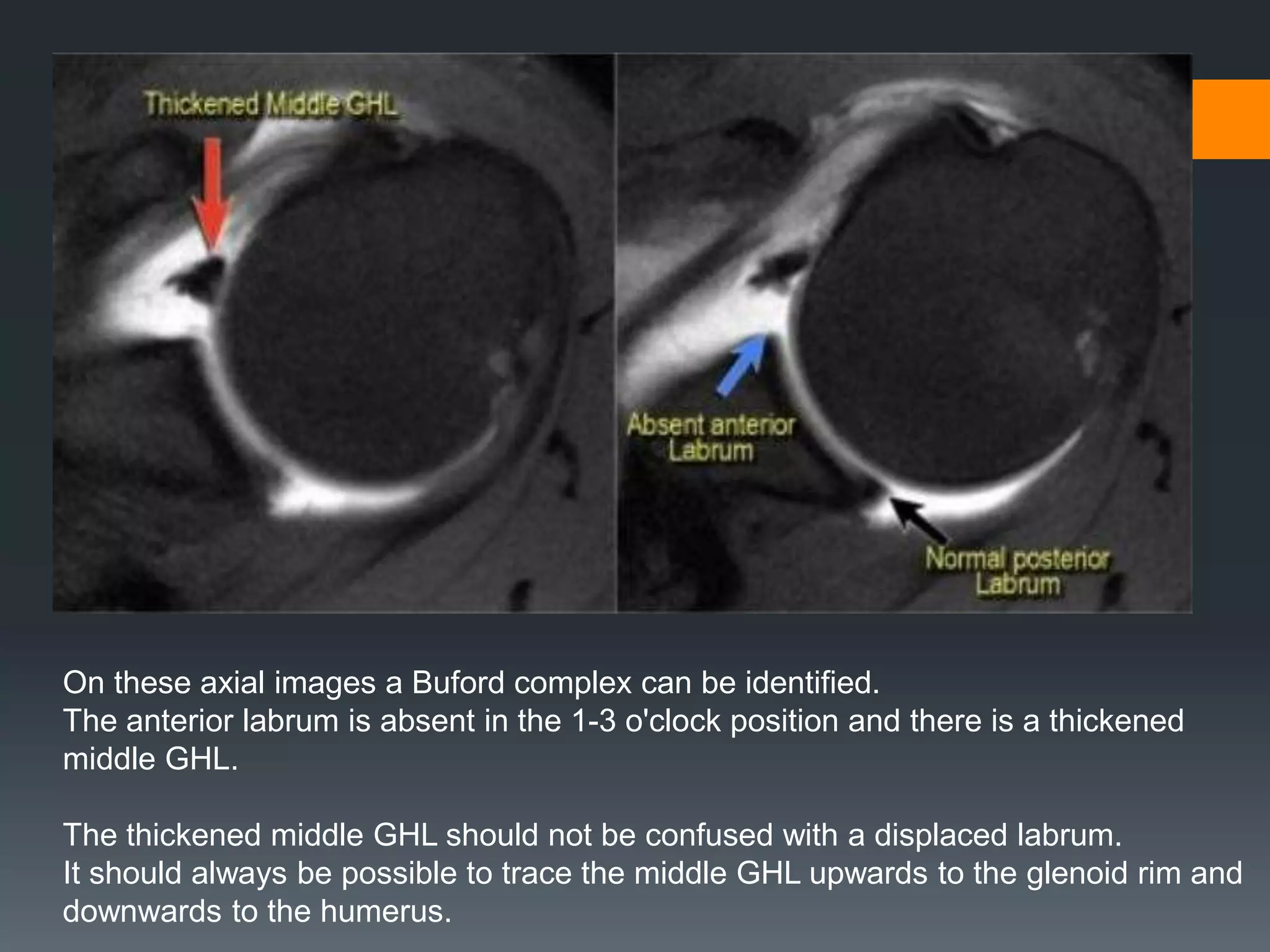
Describes labral types and conditions such as sublabral foramen and Buford complex, including their prevalence.
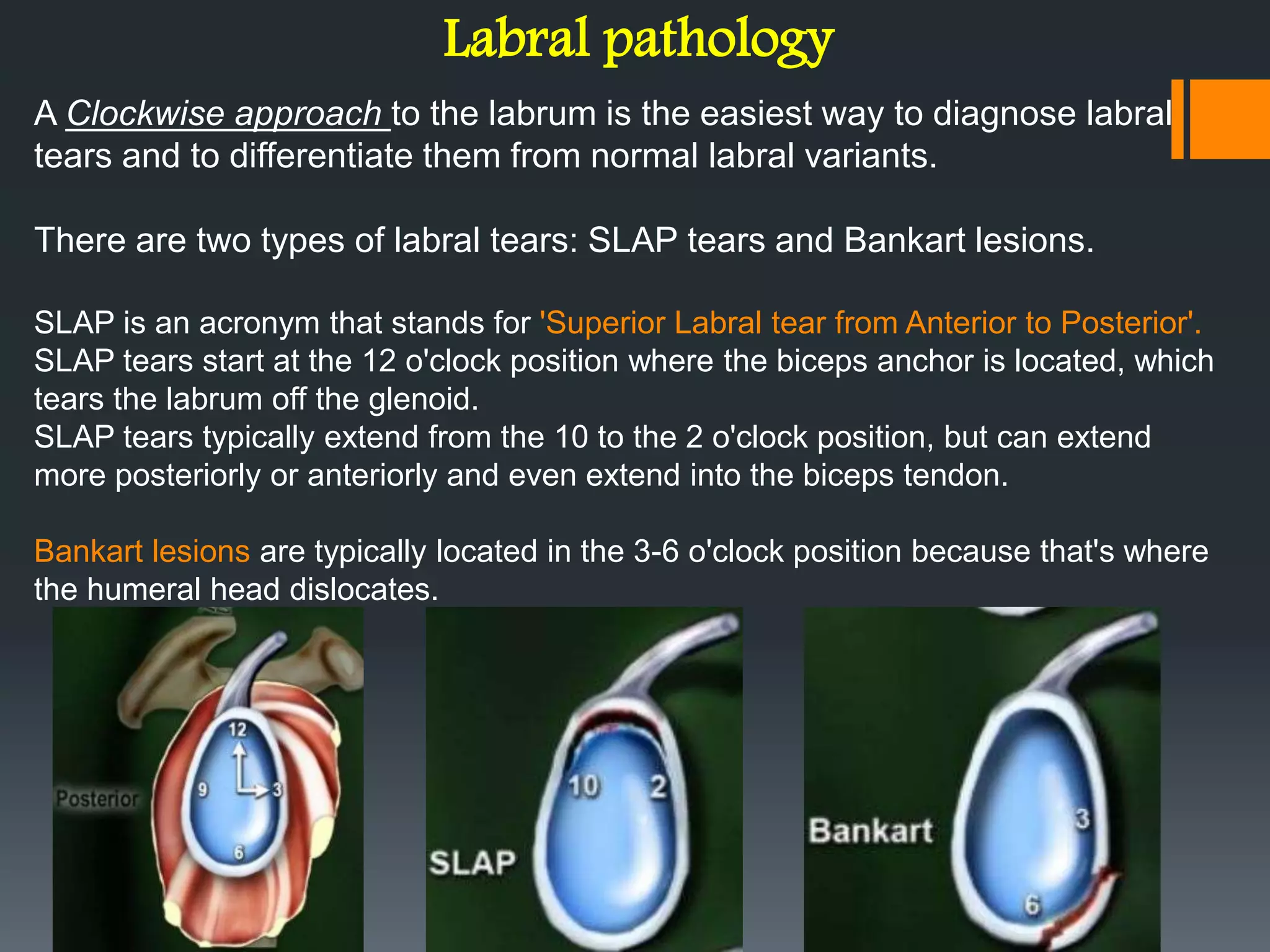
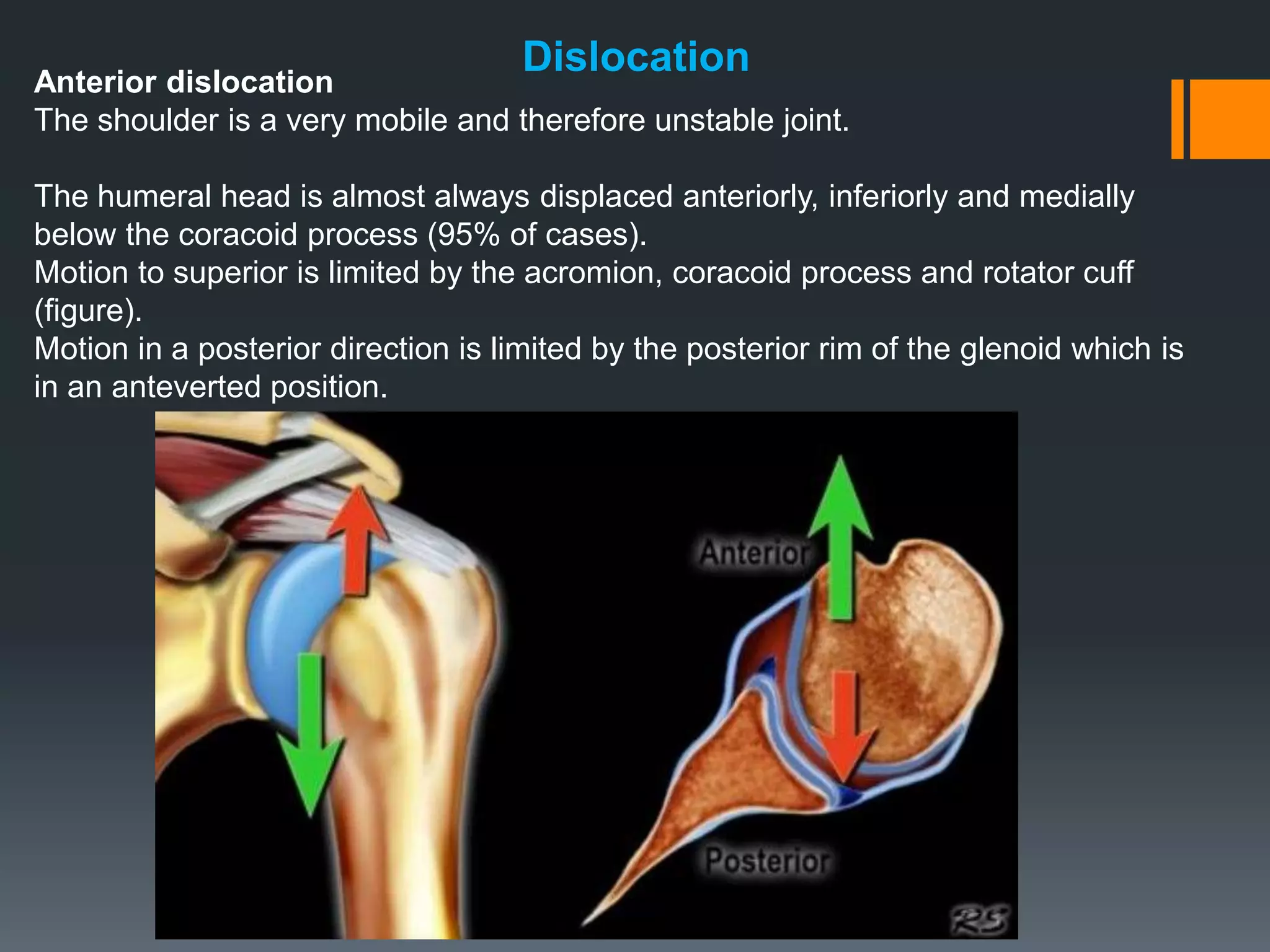
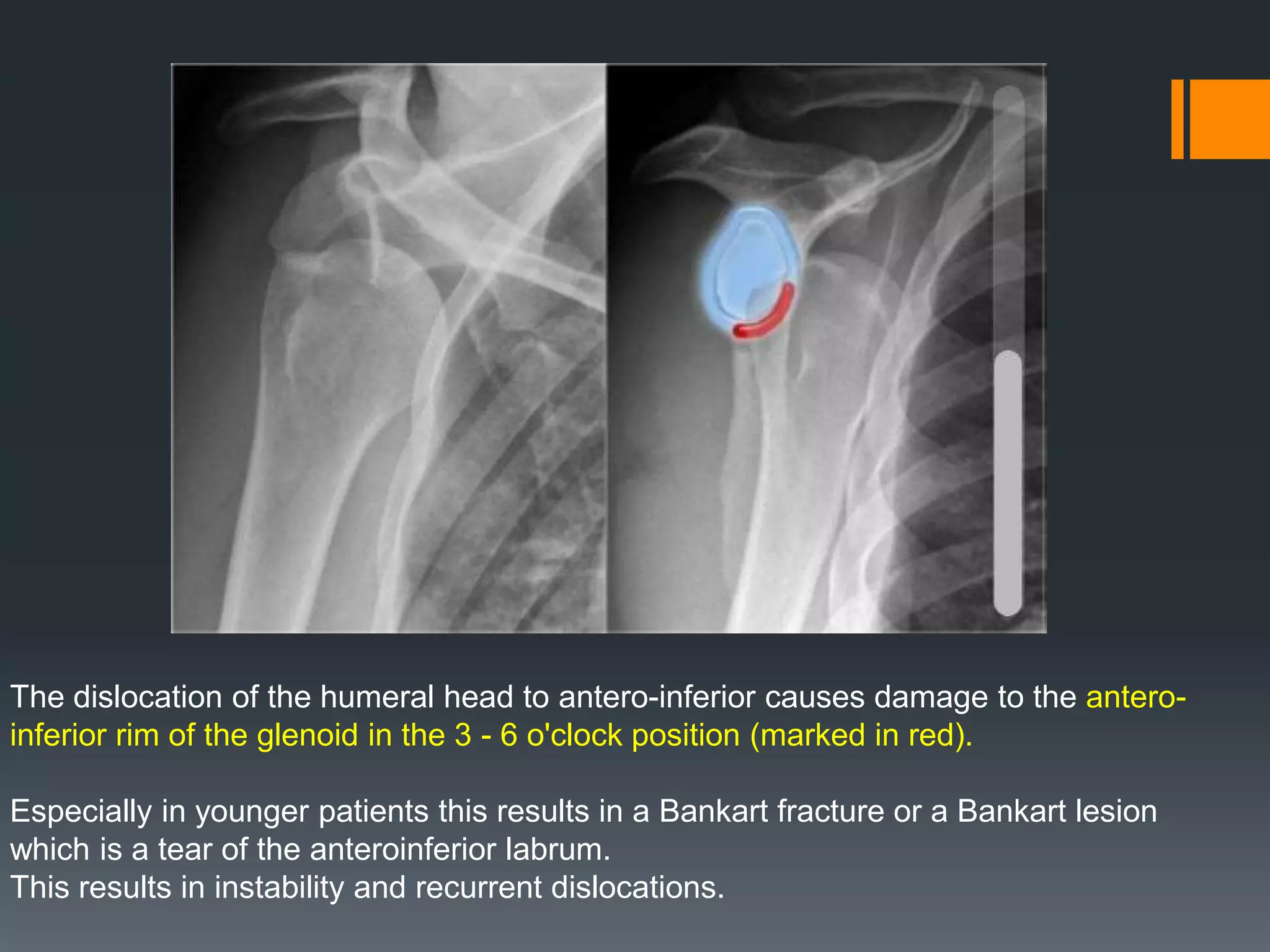
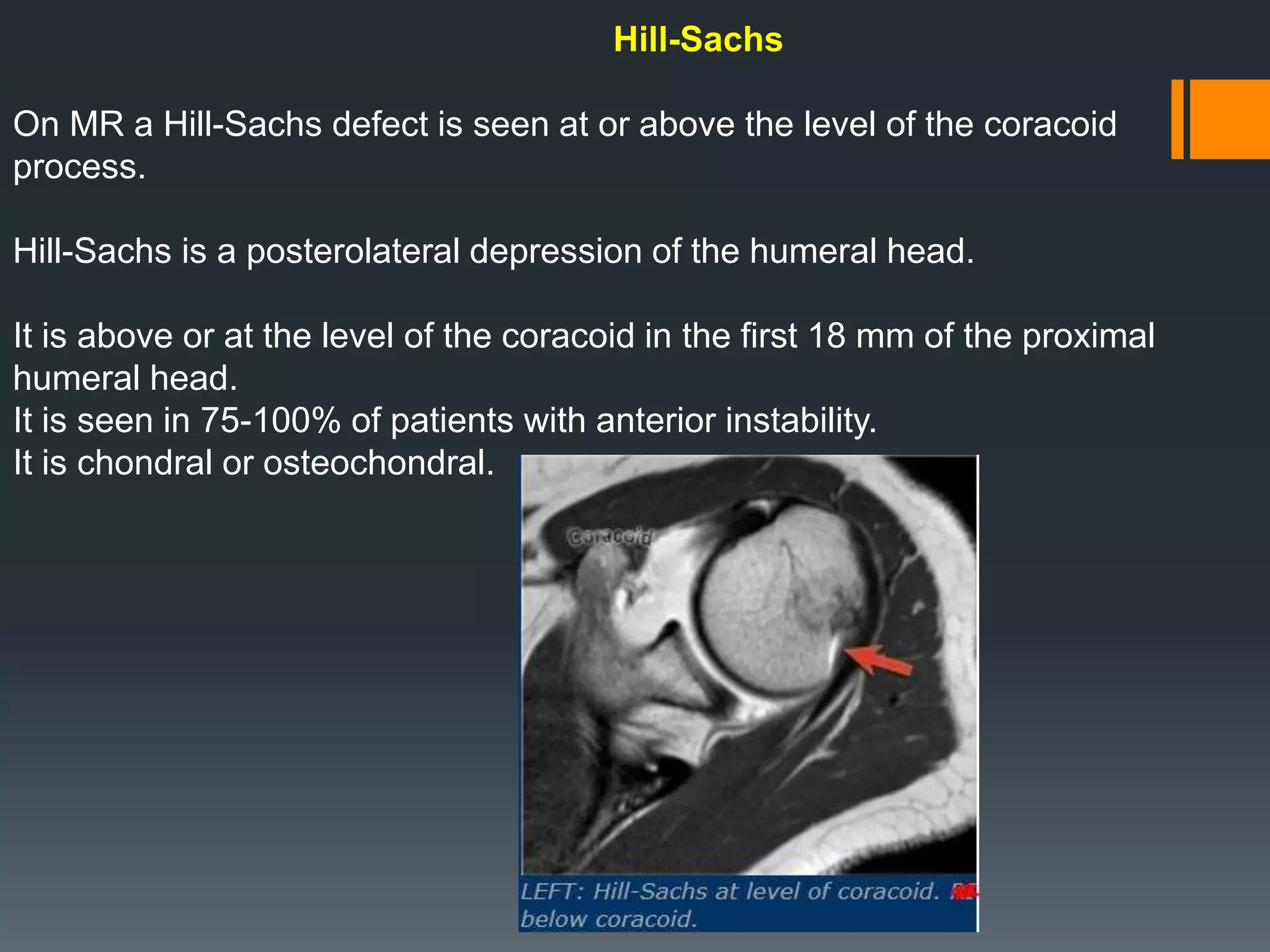
Identifies various labral pathologies, including Bankart lesions and tear types, and dislocation implications.
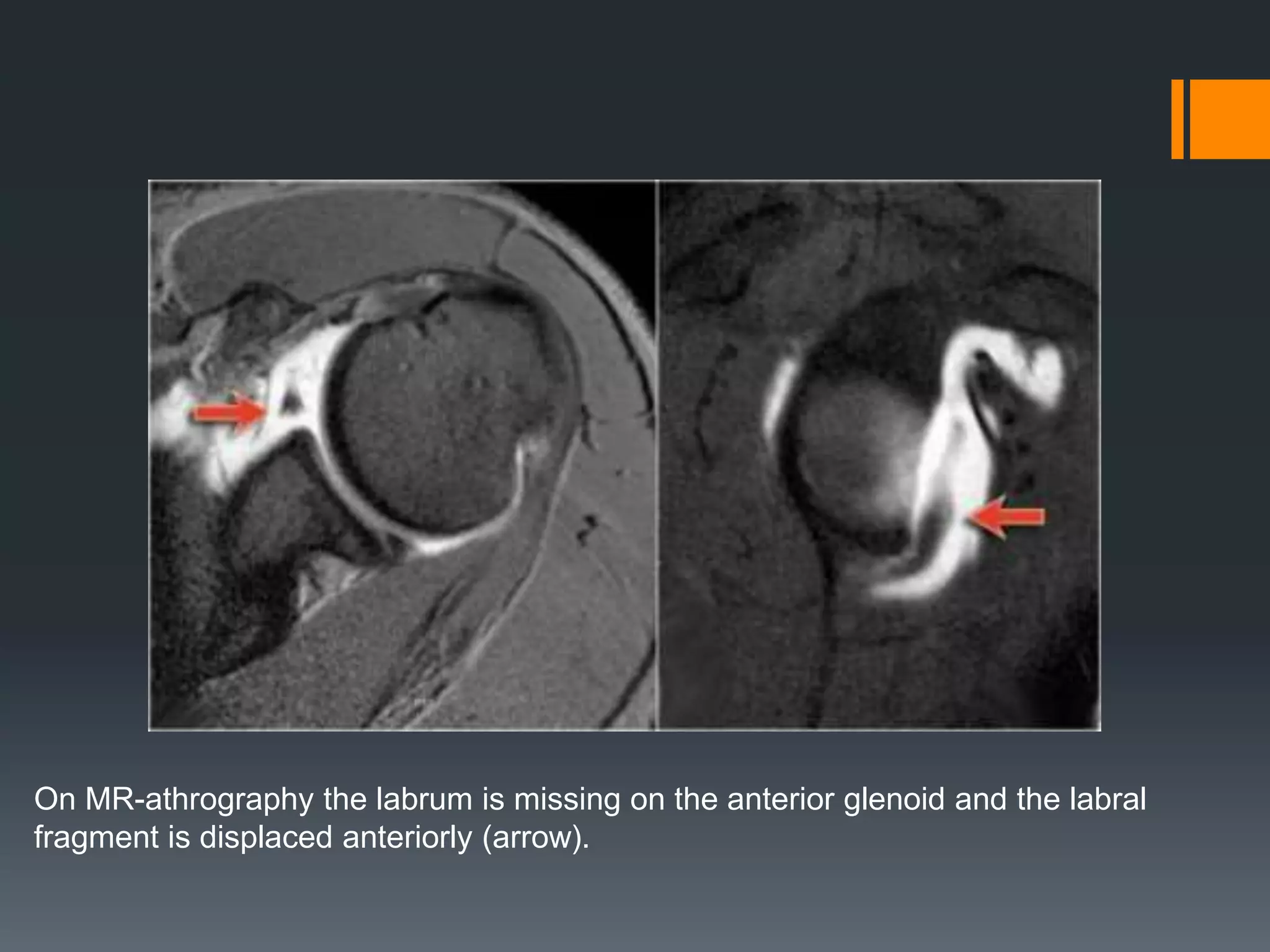
Details the identification and implications of Bankart lesions, including MRI findings and common associated conditions.
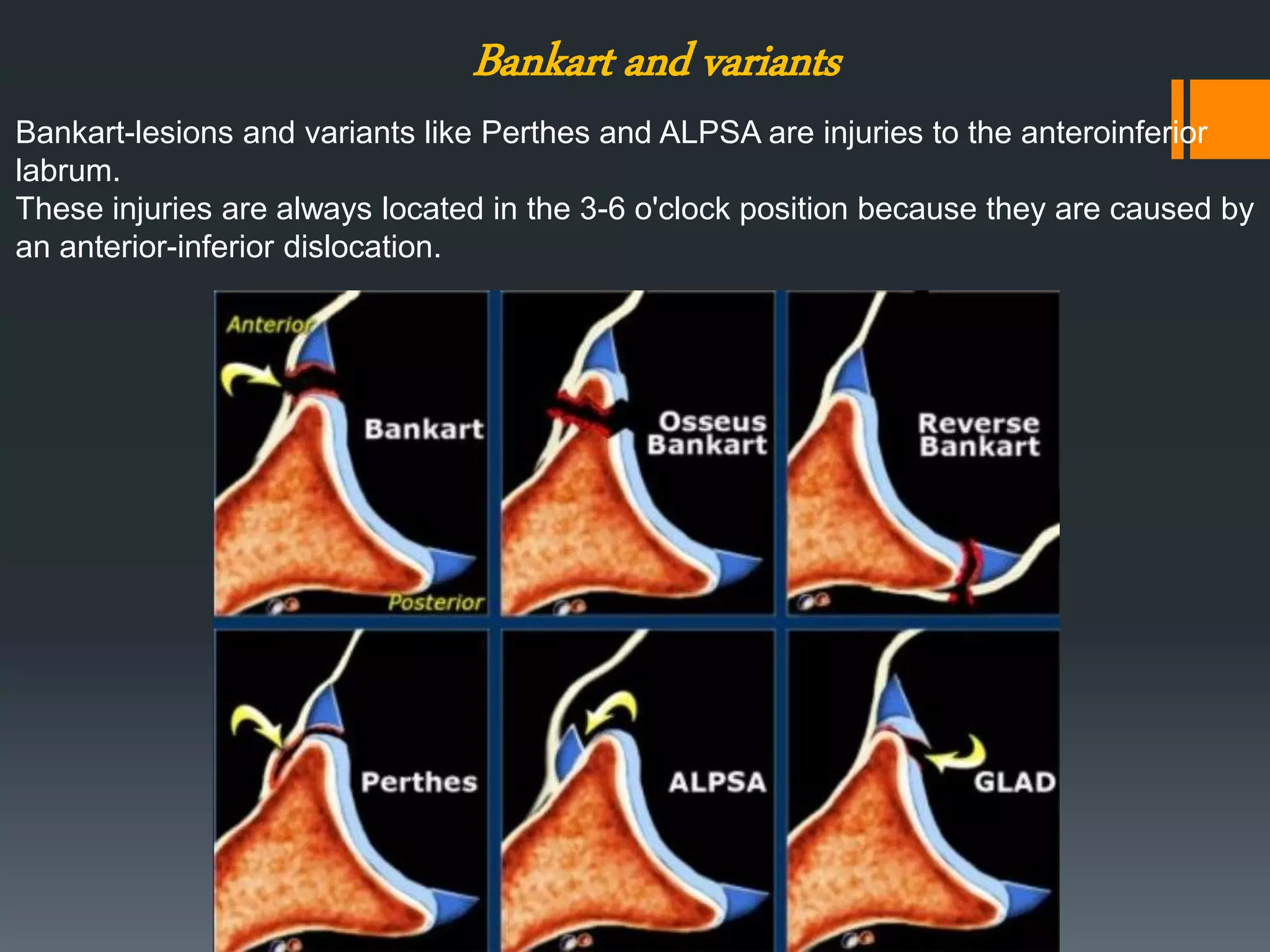
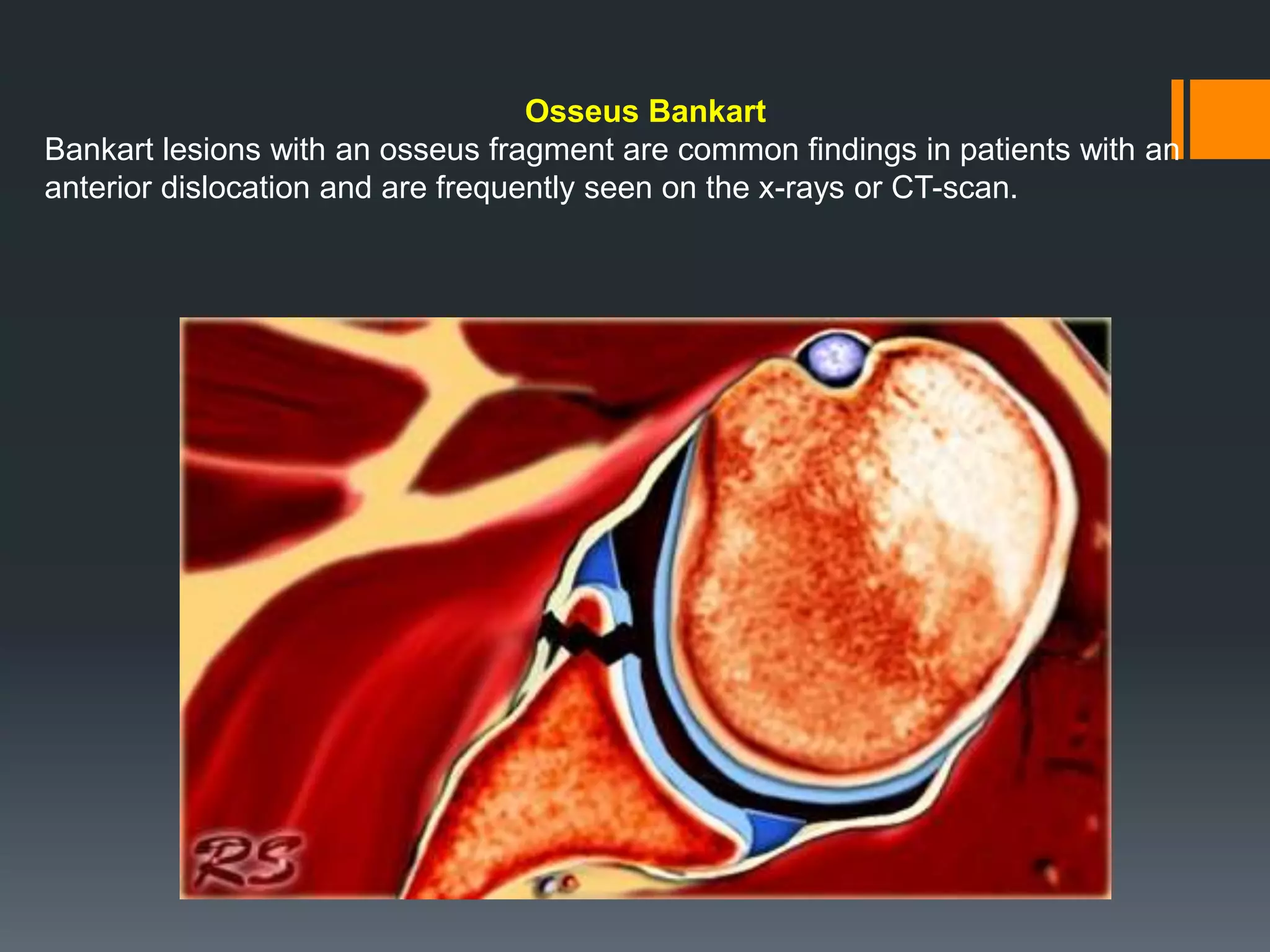
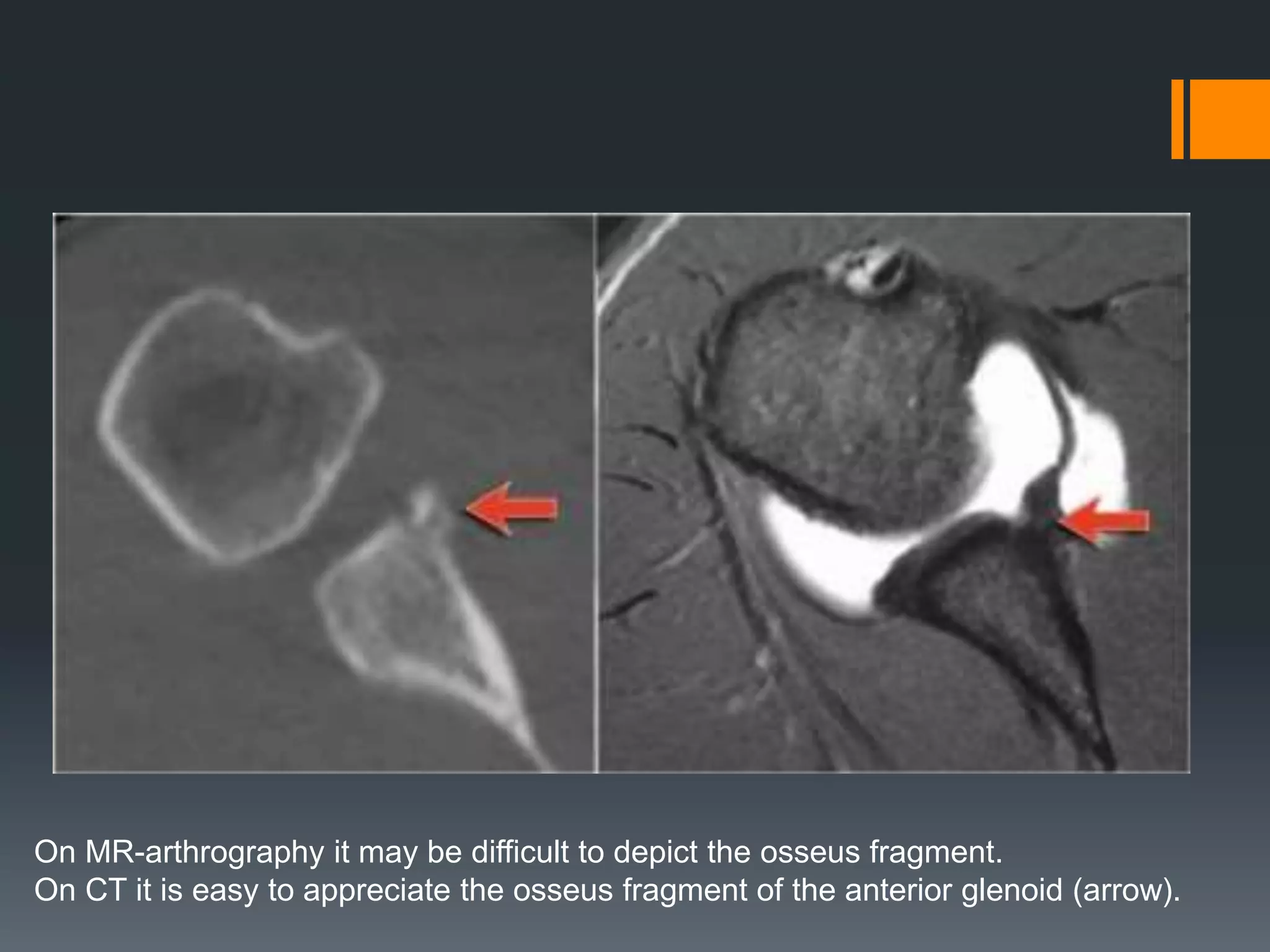
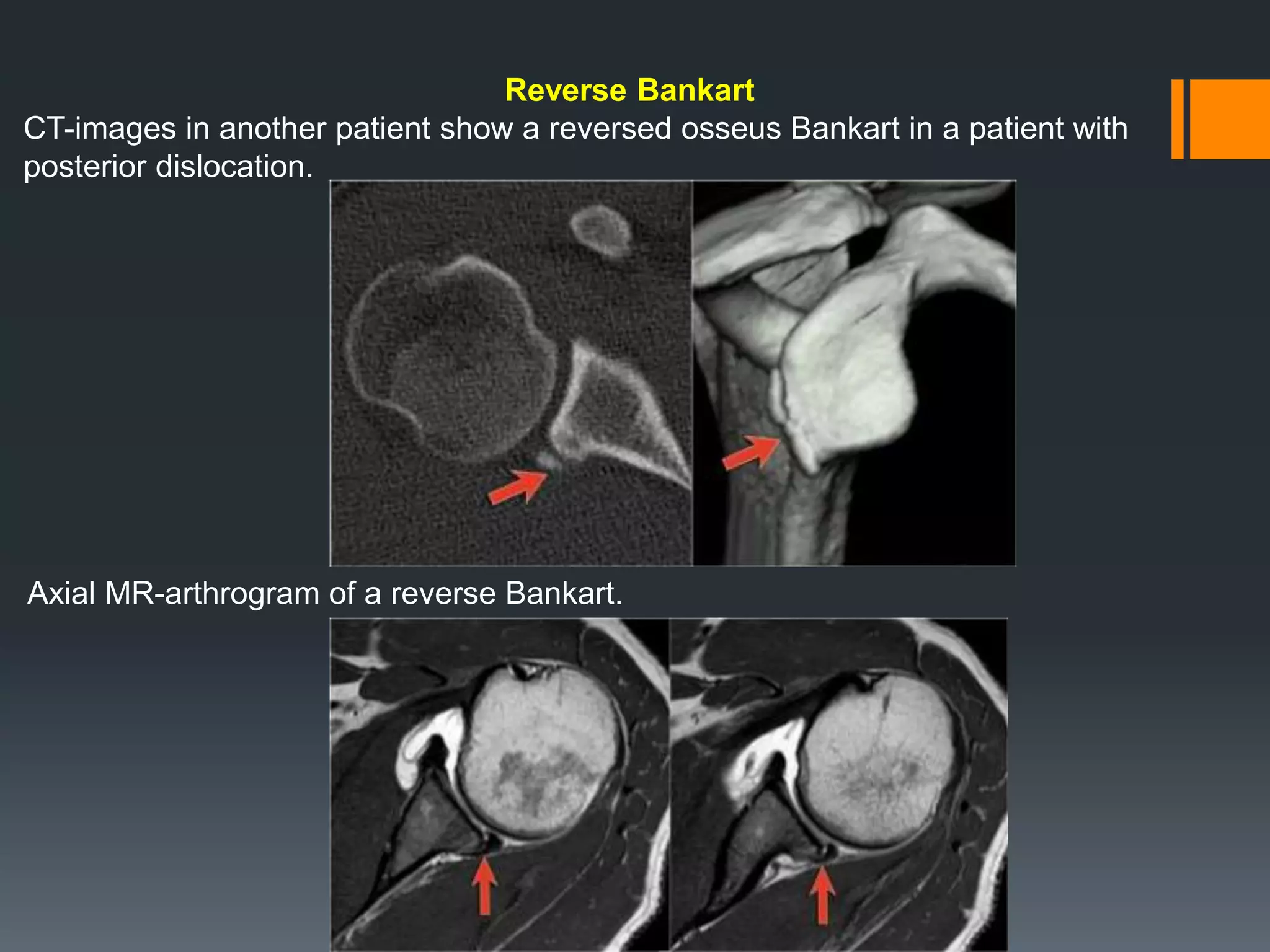
Discusses osseous Bankart lesions and reverse types, highlighting diagnostic challenges and imaging techniques.
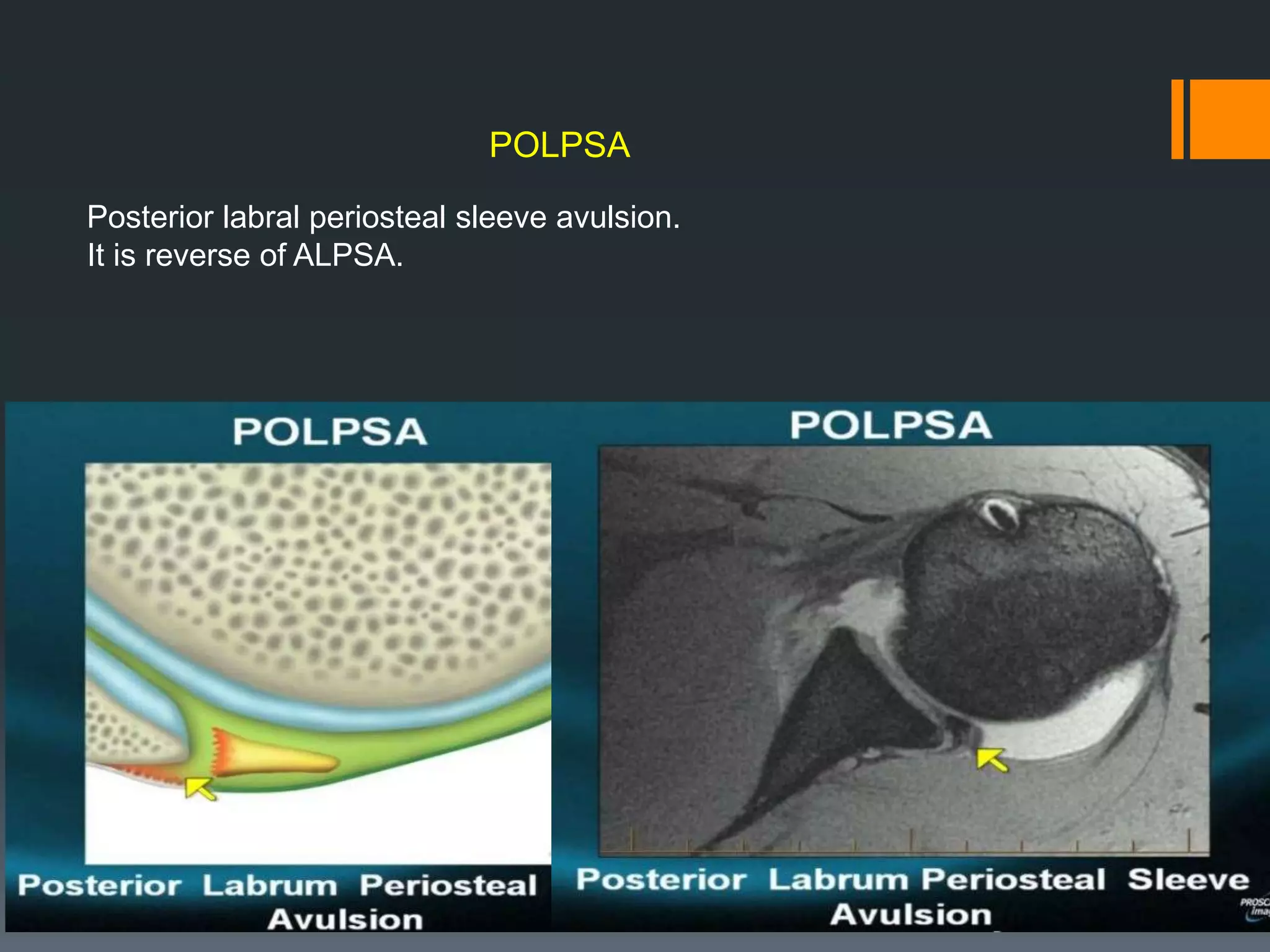
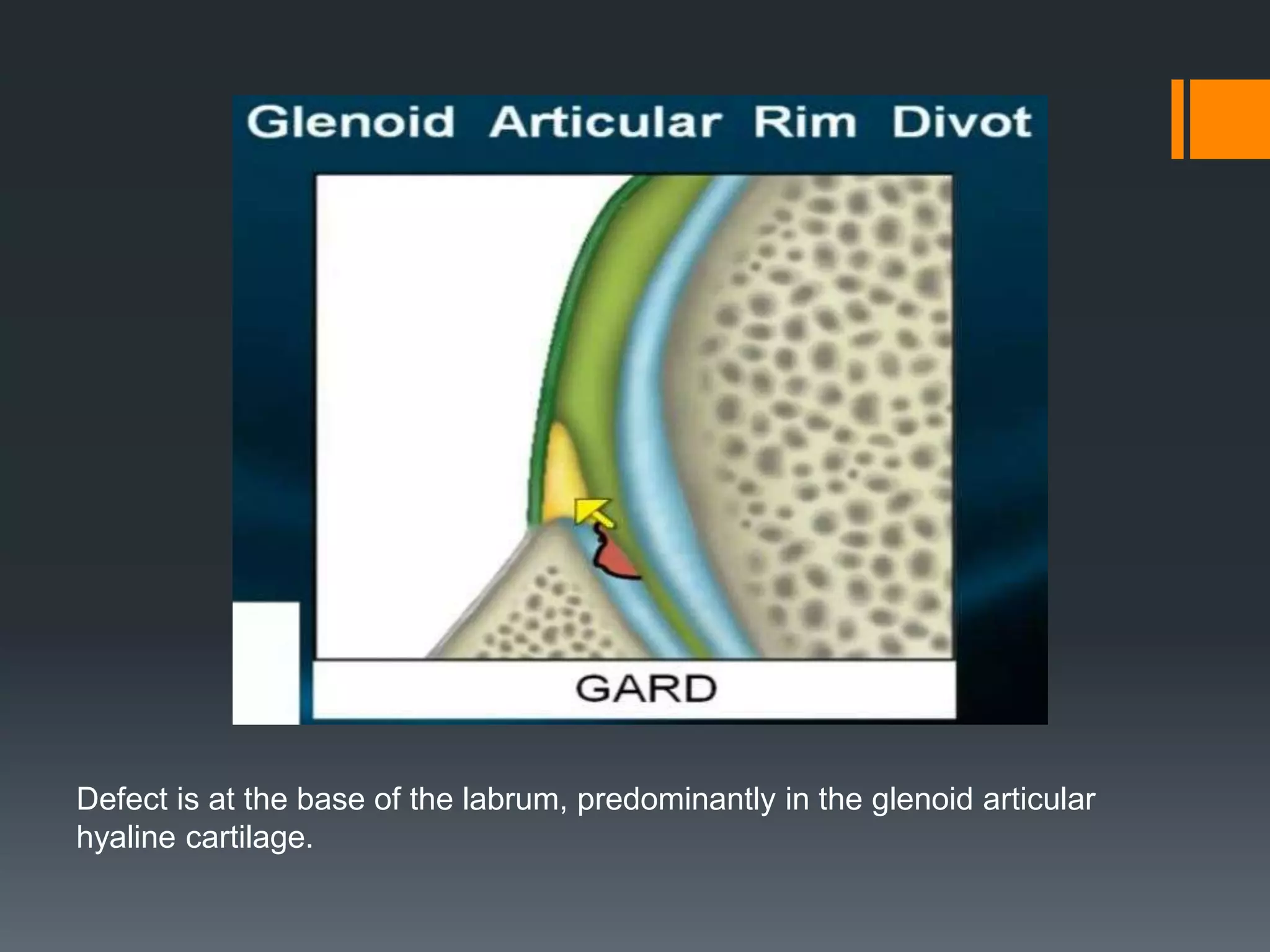
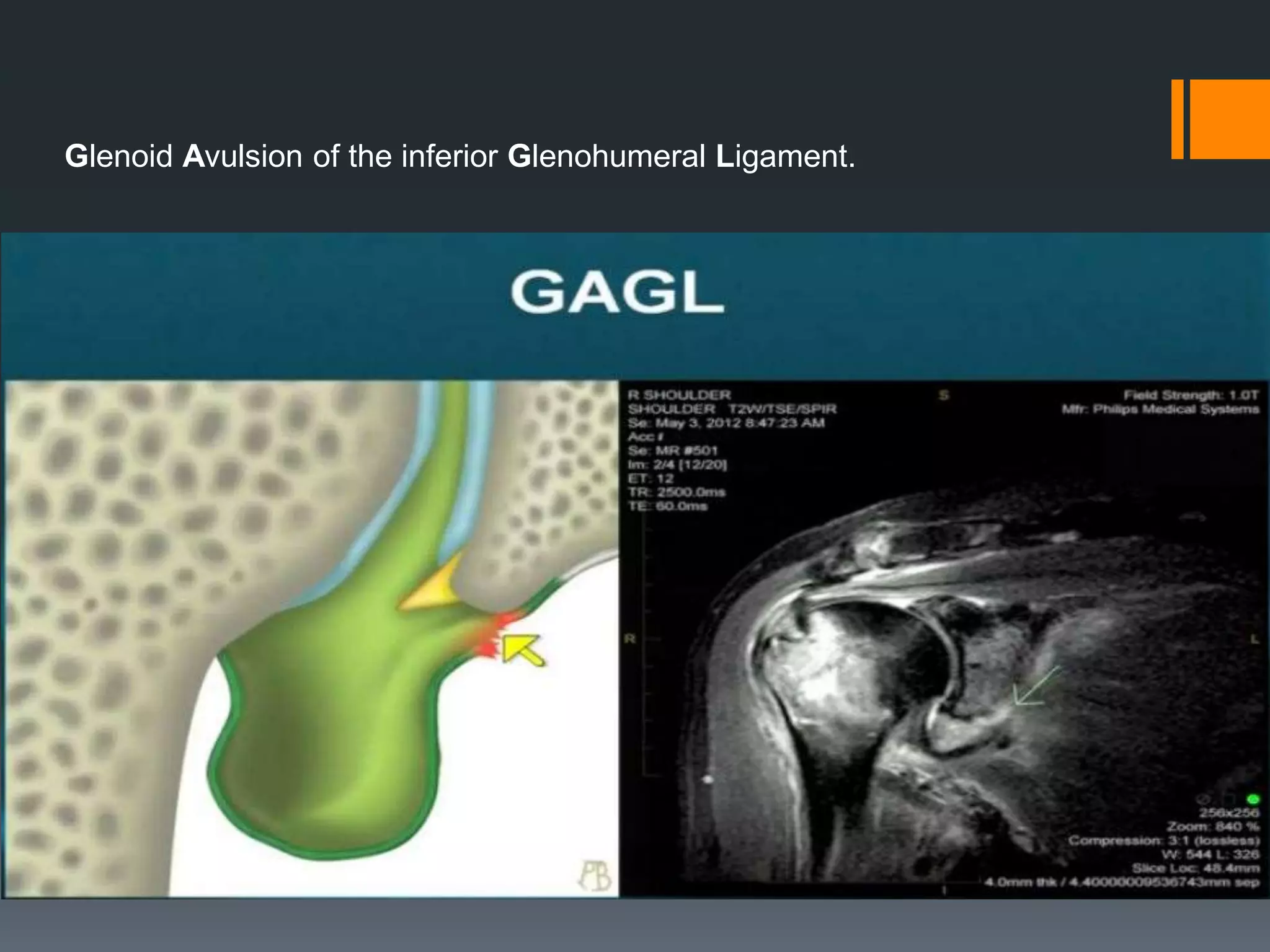
Explains ALPSA, POLPSA, and GLAD lesions as distinct pathological entities and their imaging characteristics.
Final slide thanking the audience.






























































































