Downloaded 318 times


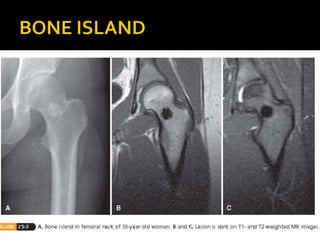






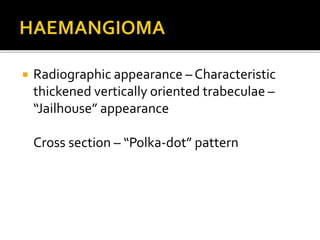



The document discusses various types of bone tumors, benign and malignant lesions, and non-neoplastic conditions, detailing their common sites, symptoms, imaging characteristics, histology, and treatment options. It covers issues ranging from osteoid osteoma and chondromas to fibrous lesions and Paget's disease, emphasizing demographics, typical presentations, and diagnostic measures. The text serves as a comprehensive overview for medical professionals in orthopaedic surgery to understand the complexities of bone pathology.


















































































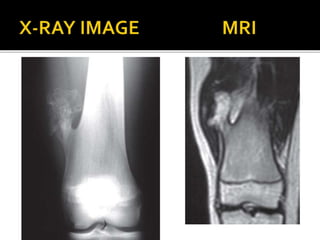
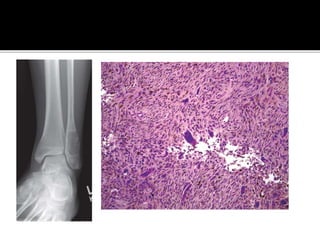
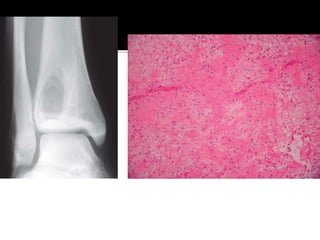
![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




