Downloaded 632 times
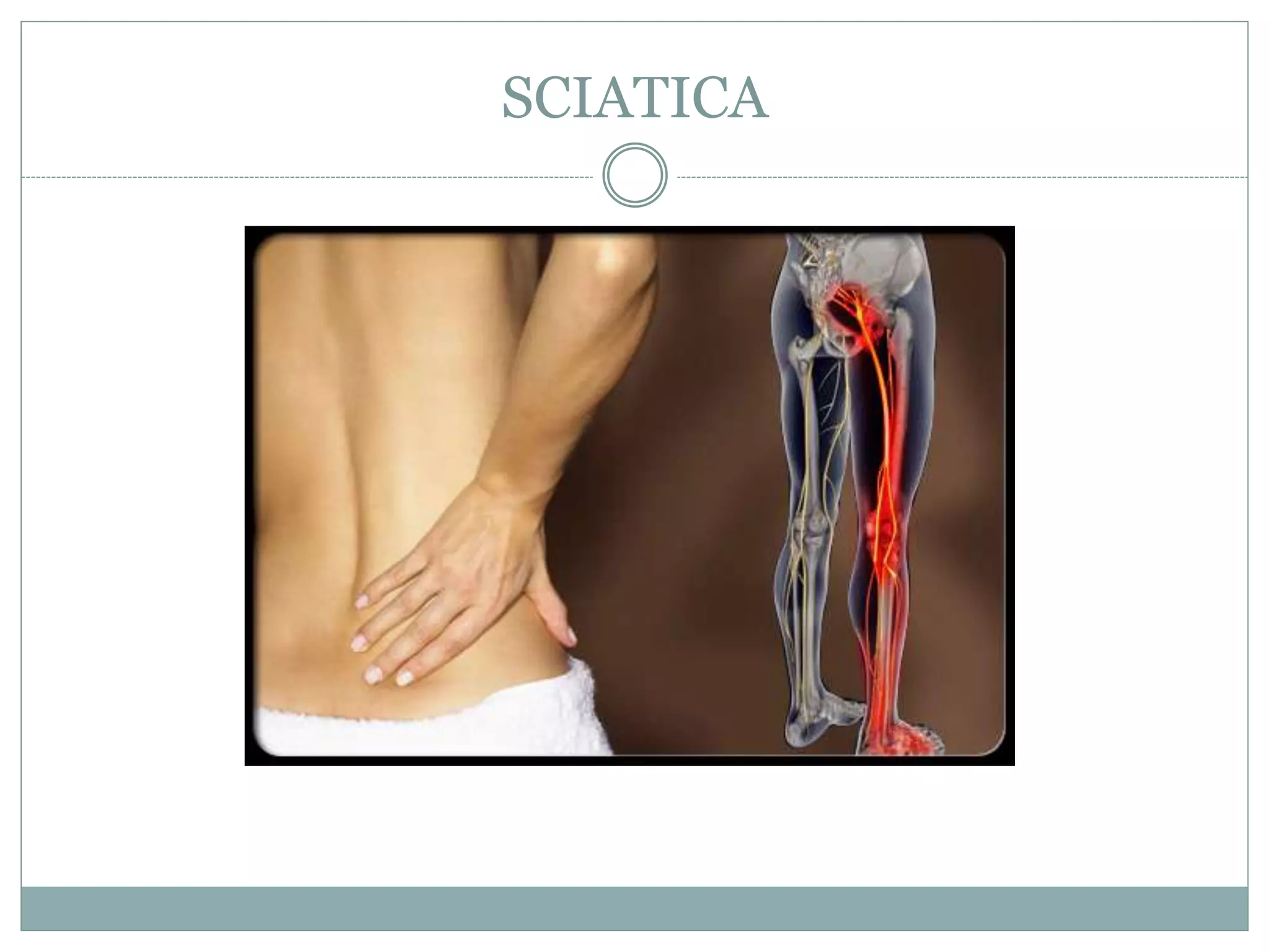










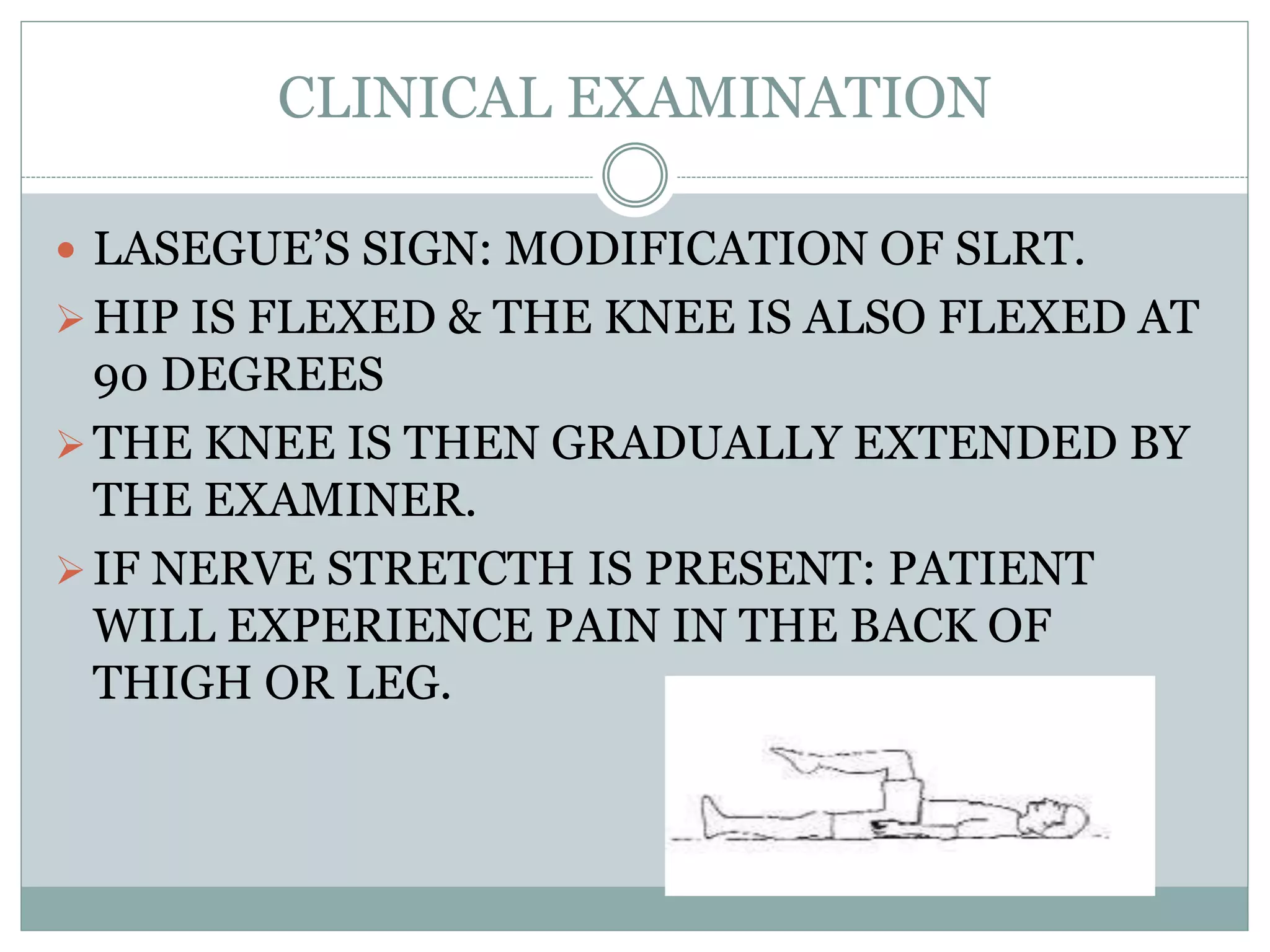
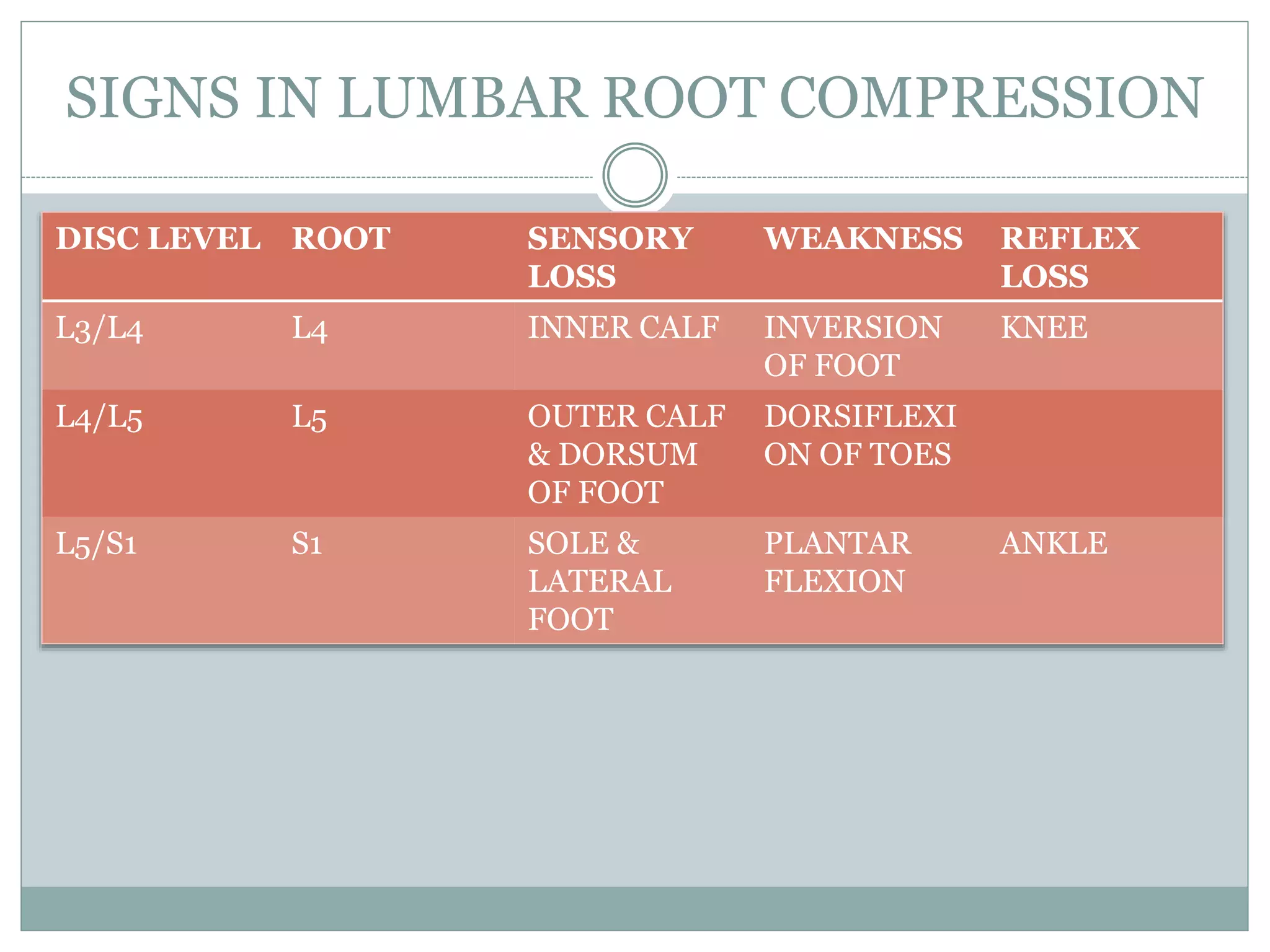















Sciatica is a common radiating pain syndrome caused by irritation of the sciatic nerve root, usually from a herniated disc at L4-L5 or L5-S1. It presents as low back pain radiating down the back of the leg and can affect the foot. Sciatica is a symptom rather than a diagnosis. Examination may reveal a positive straight leg raise test. Differential diagnoses include spondyloarthropathies. Imaging like MRI can identify disc herniations while conservative treatments include rest, analgesics, and epidural injections. Surgery is considered if conservative options fail or neurological deficits are present.