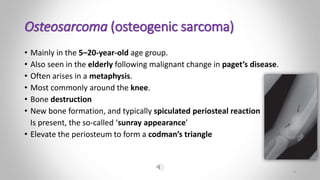
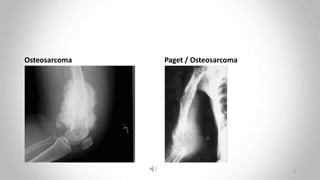
- Osteosarcoma most commonly arises in the metaphysis around the knee in children and young adults. MRI is most accurate for showing tumor extent using multiplanar views. It presents as bone destruction, new bone formation and a sunray periosteal reaction.
- Chondrosarcoma mainly affects those aged 30-50 and most commonly involves the pelvis, scapulae, humerus and femur. It appears as a lytic expanding lesion containing flecks of calcium. Pelvic chondrosarcomas often have large soft tissue components.
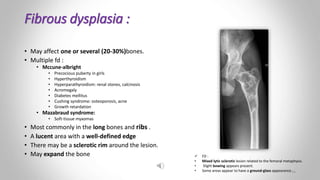
- Fibrous dysplasia may affect one or several bones and most commonly involves the long bones and ribs. It appears as a lu