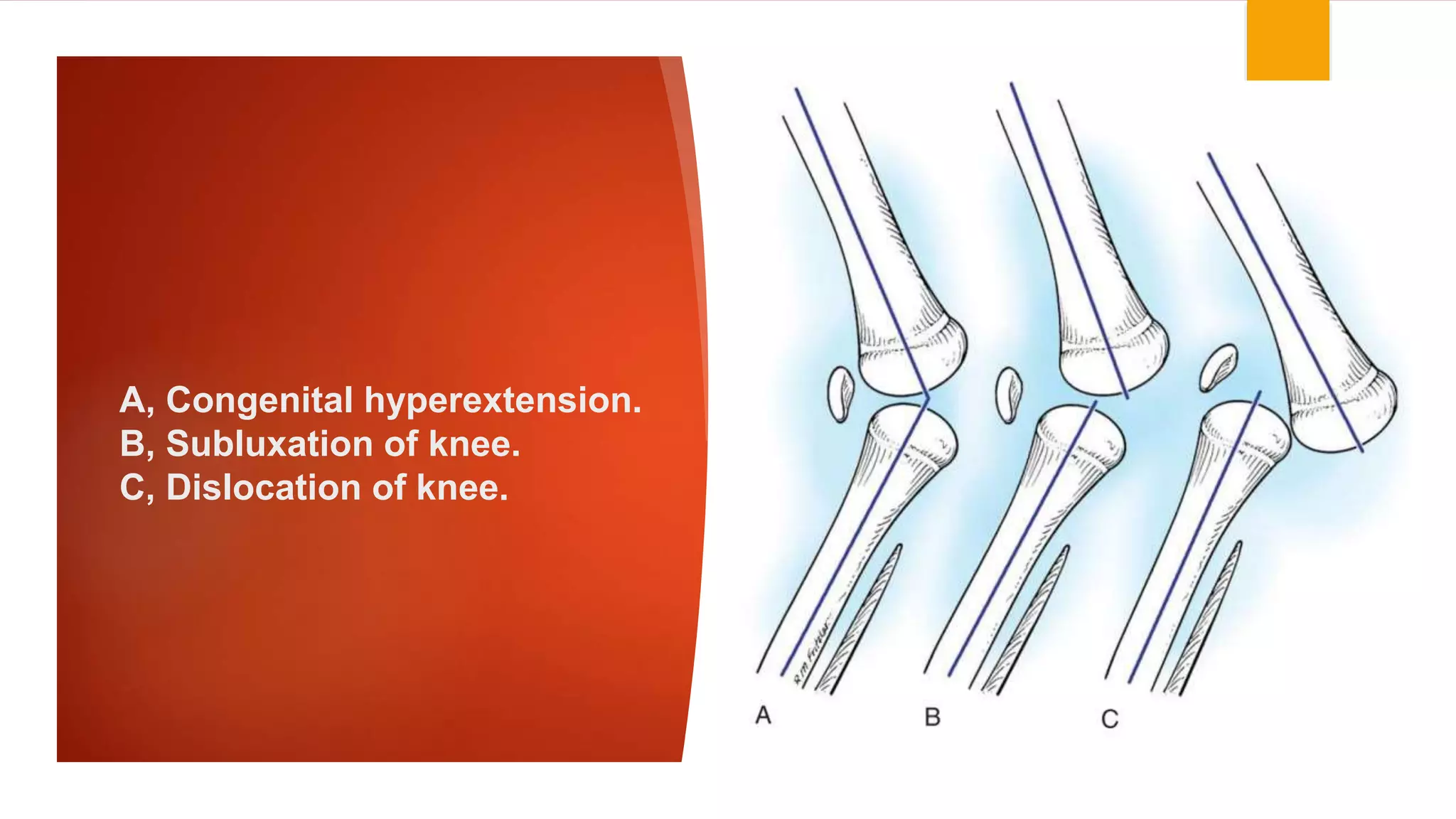
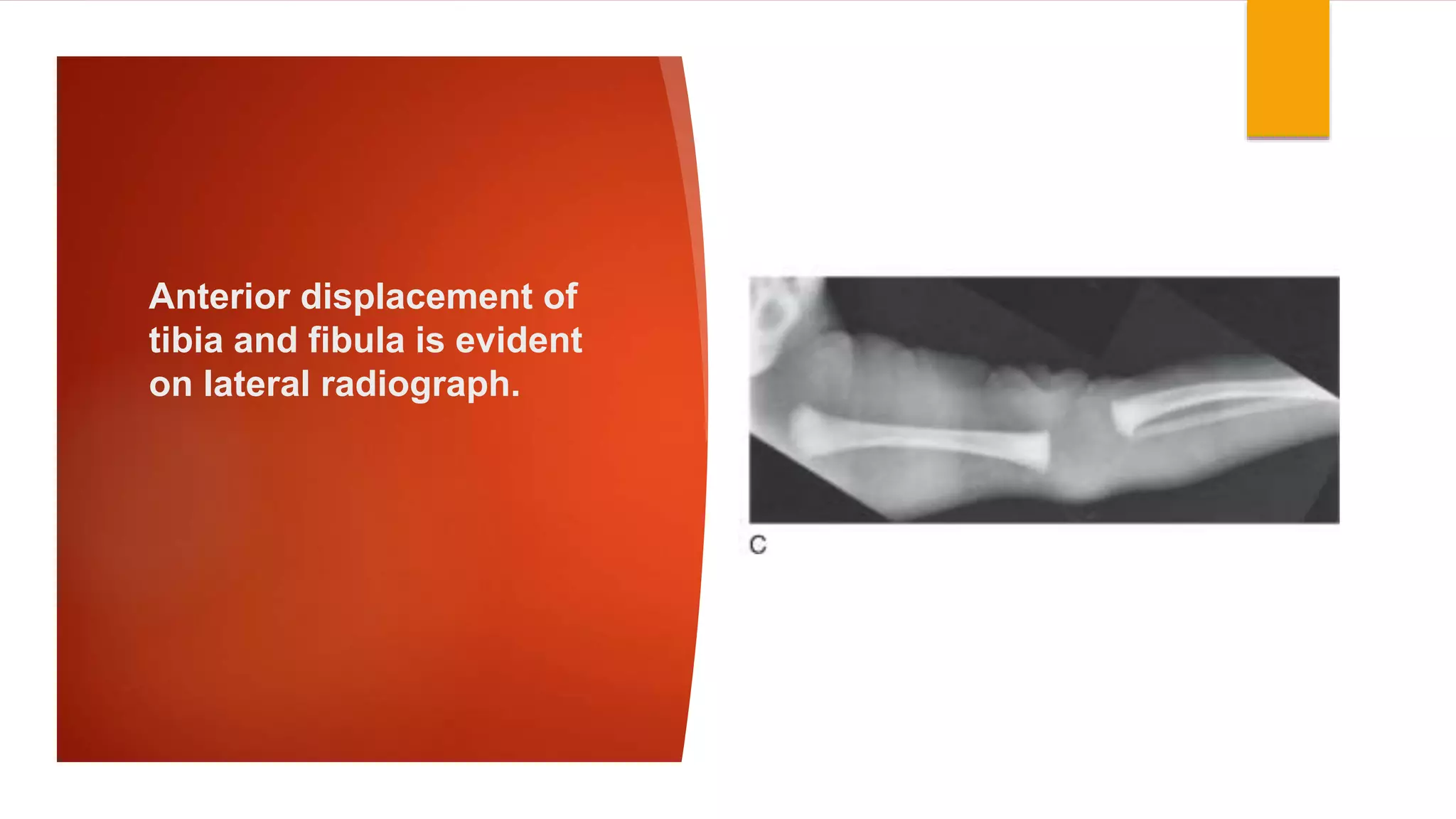
This document discusses congenital hyper extension and dislocation of the knee. It begins with an introduction describing the spectrum of the condition from positional contractures to rigid dislocation. It is often associated with other developmental hip and foot conditions. Structurally, the anterior knee capsule and quadriceps mechanism are contracted. Clinically, it presents with a hyperextended knee at birth. Treatment depends on severity, with non-operative treatment using casting for mild cases and surgical release for more severe or non-responsive cases.