Downloaded 103 times
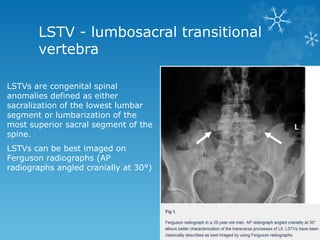

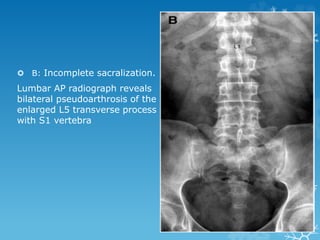
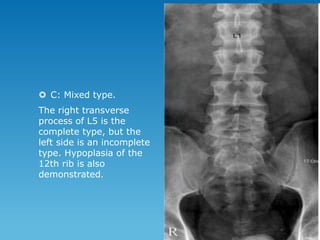
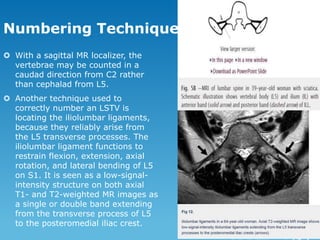

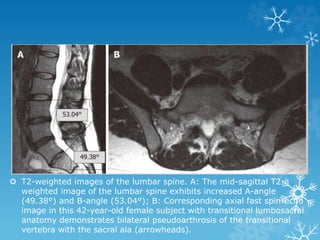


This document discusses lumbosacral transitional vertebrae (LSTV), which are congenital spinal anomalies involving sacralization of the lowest lumbar segment or lumbarization of the highest sacral segment. LSTVs can be classified based on imaging features and involve fusion of the transverse process to the sacrum. Numbering the vertebrae can be challenging with LSTVs. Prediction of LSTVs on MRI is possible based on increased A and B angles on sagittal images, which measure the inclination of the sacrum and lumbar lordosis. LSTVs can cause low back pain known as Bertolotti syndrome through various mechanisms.











































































































