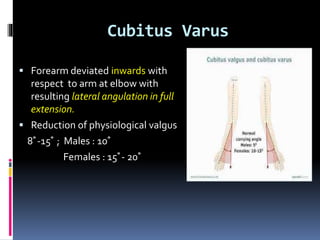
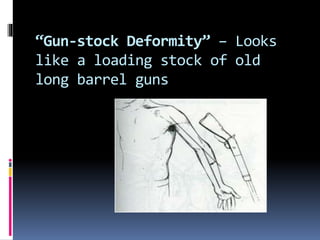
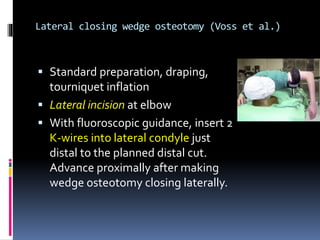
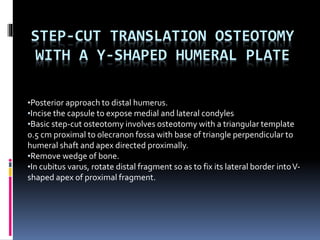
This document discusses cubitus varus, which is a deformity where the forearm is deviated inward at the elbow joint, reducing the normal valgus angle. It describes the causes, types, clinical examination findings, measurements on x-rays, and treatment options. The most common treatment involves corrective osteotomy, with various techniques described such as lateral closing wedge osteotomy, medial open wedge osteotomy, oblique osteotomy, and dome osteotomy. Complications of osteotomy include stiffness, nerve injury, persistent or recurrent deformity, non-union, and skin issues.