Downloaded 131 times
























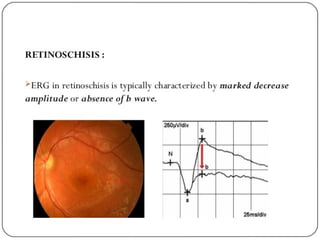





Retinoschisis is a splitting of the neurosensory retina into inner and outer layers, causing visual field defects. Senile retinoschisis occurs in 5% of people over 20 and presents as bilateral, peripheral retinal elevations that may progress circumferentially. Juvenile retinoschisis is an X-linked condition causing macular schisis and peripheral retinoschisis from birth, leading to progressive vision loss over decades. Both types are generally asymptomatic aside from visual field defects but may develop complications like retinal detachment, vitreous hemorrhage, or neovascularization. Diagnosis involves OCT, FA, and ERG and management focuses on complications or calcium channel blockers for macular schisis























































































