Downloaded 284 times
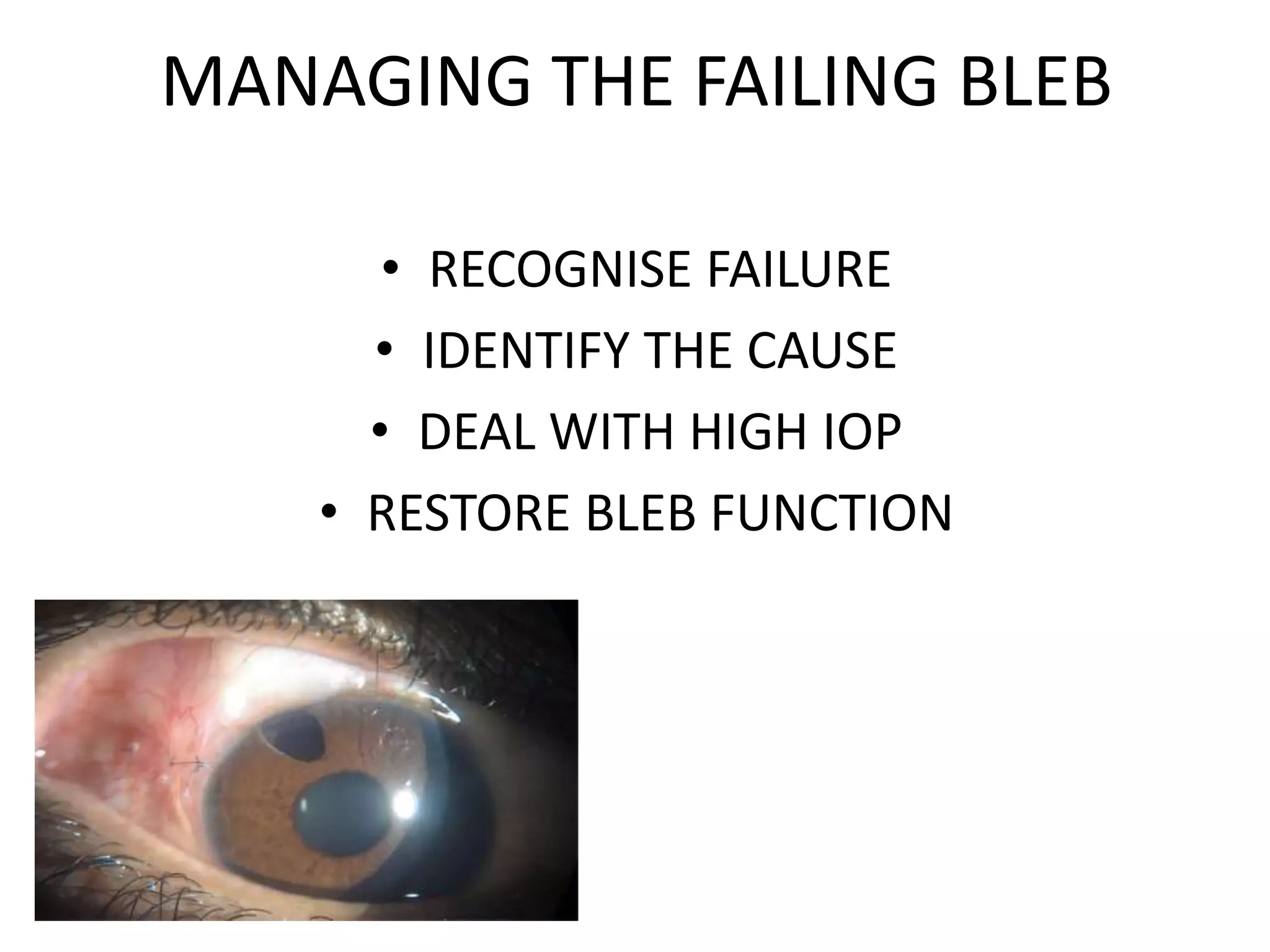
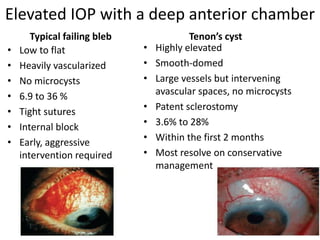
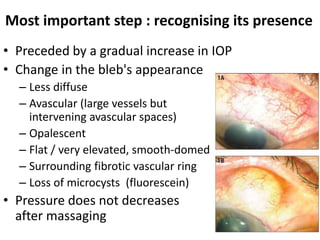


This document provides guidance on managing failing blebs after glaucoma surgery. It discusses risk factors for bleb failure, the histology of functioning vs failed blebs, typical appearances of failed blebs, identifying the cause of failure as internal or external blockage, and various management techniques. These include increasing digital pressure, medications, laser suture lysis, and bleb needling with or without anti-metabolites like mitomycin C or 5-fluorouracil to restore bleb function and control intraocular pressure. Complications of bleb needling are also reviewed.