Download to read offline




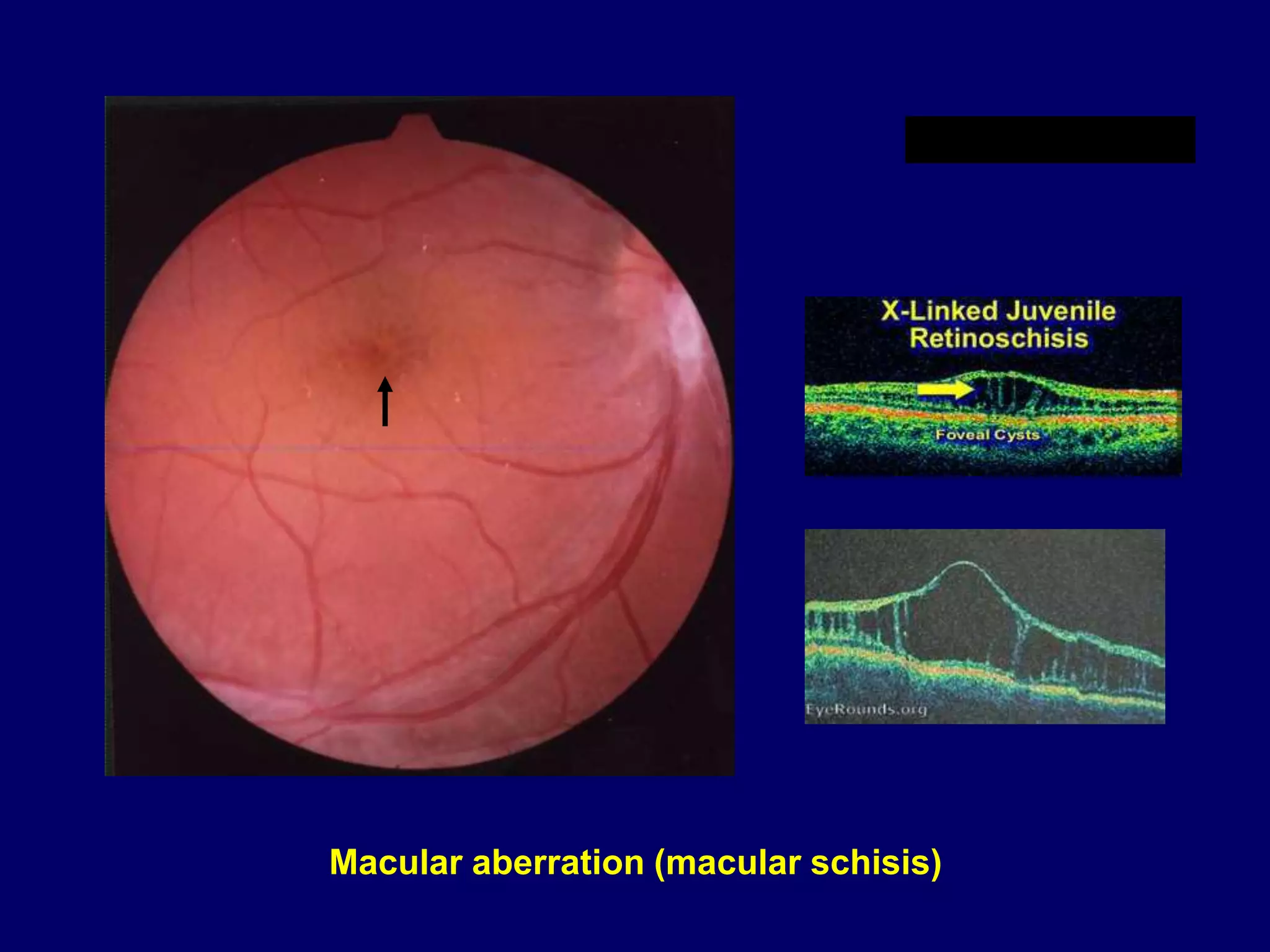

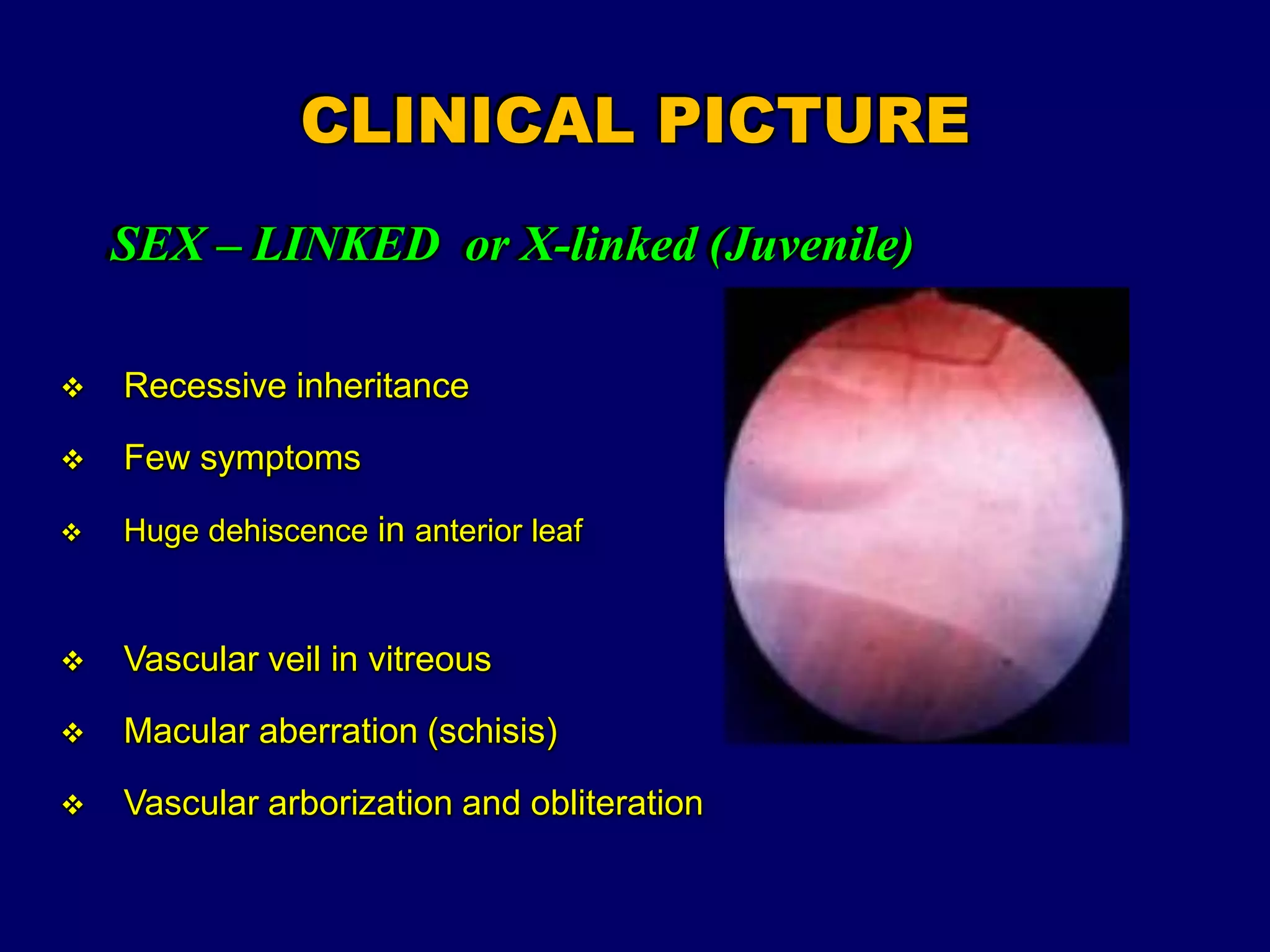



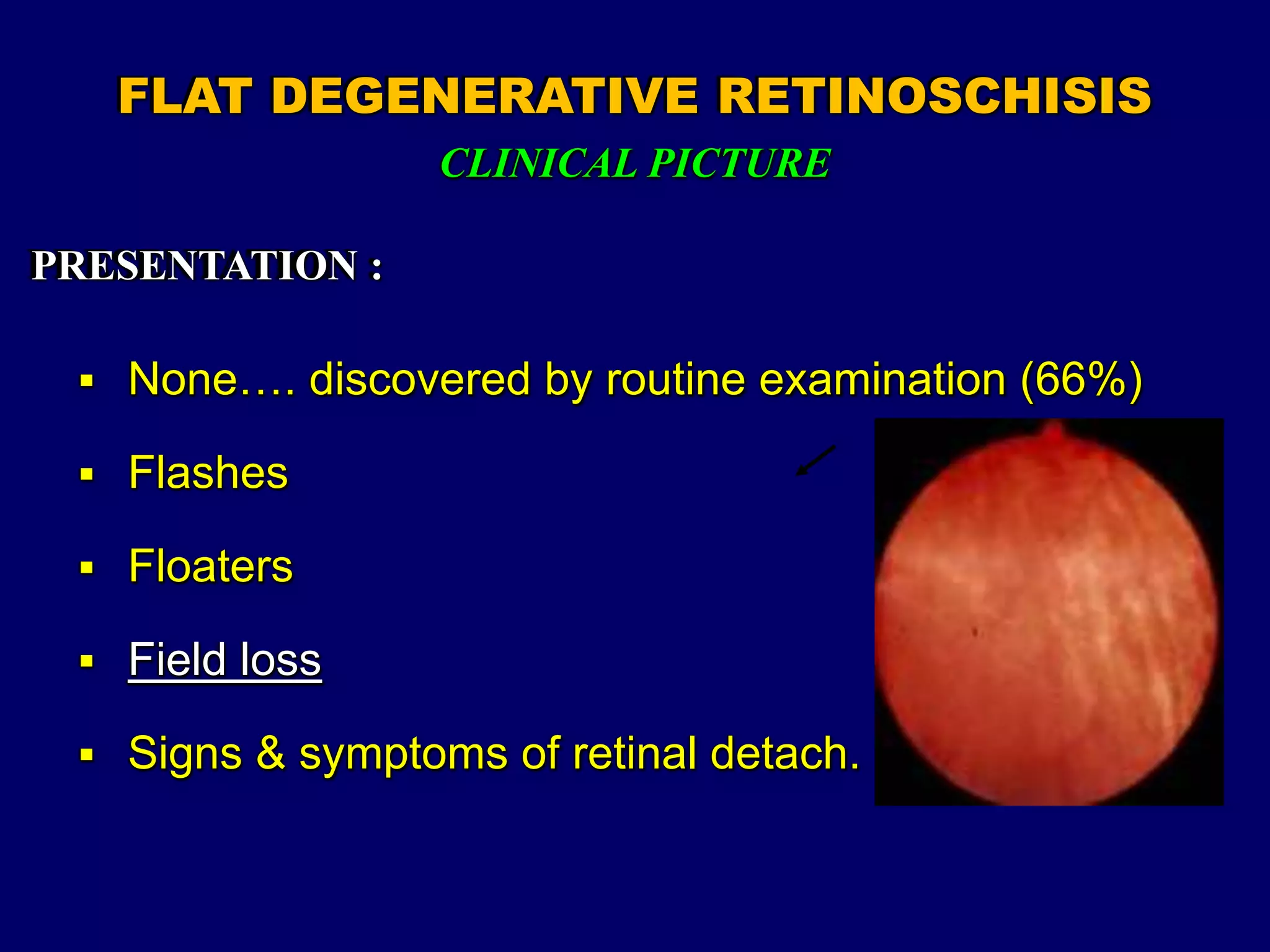





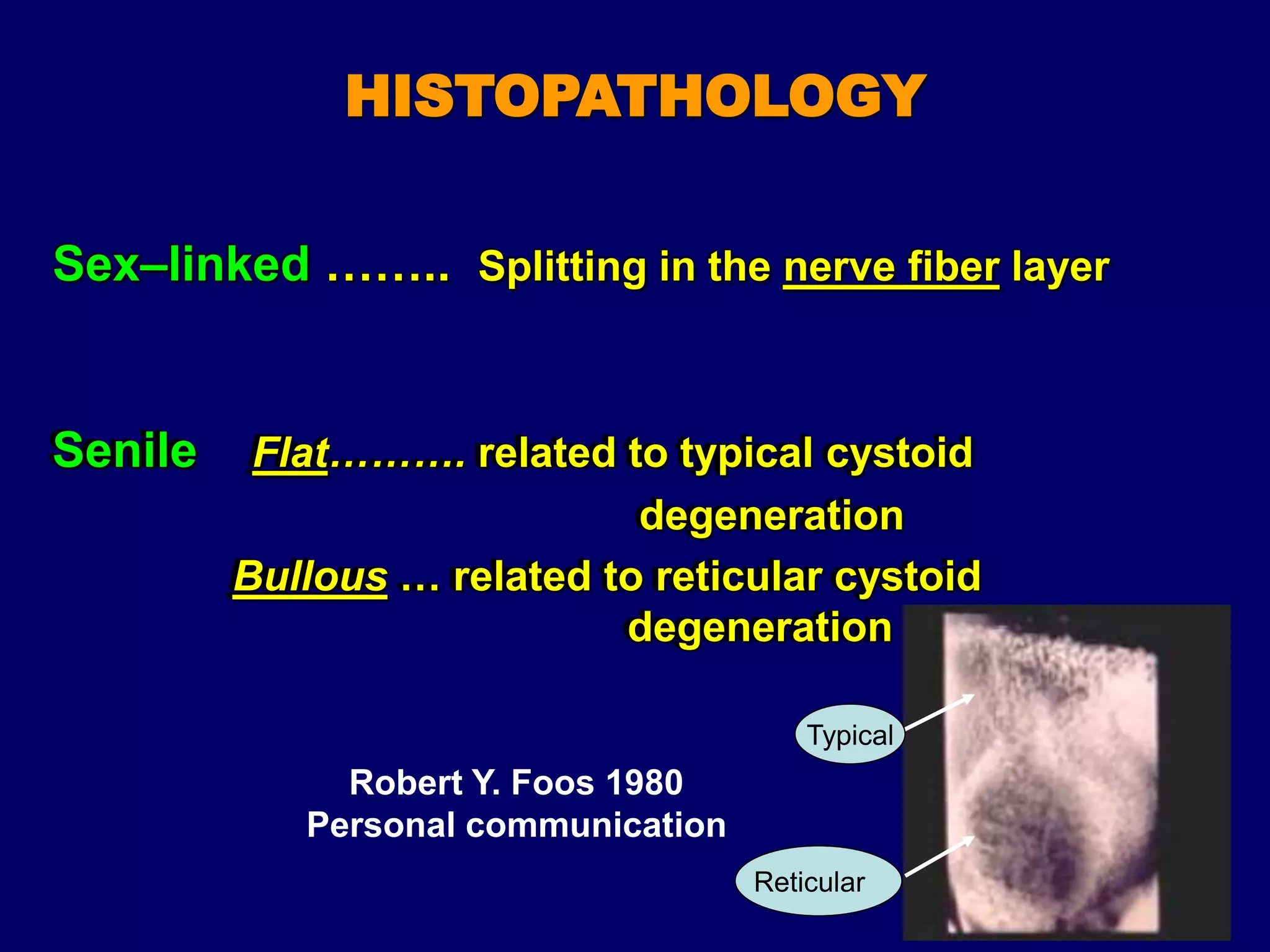



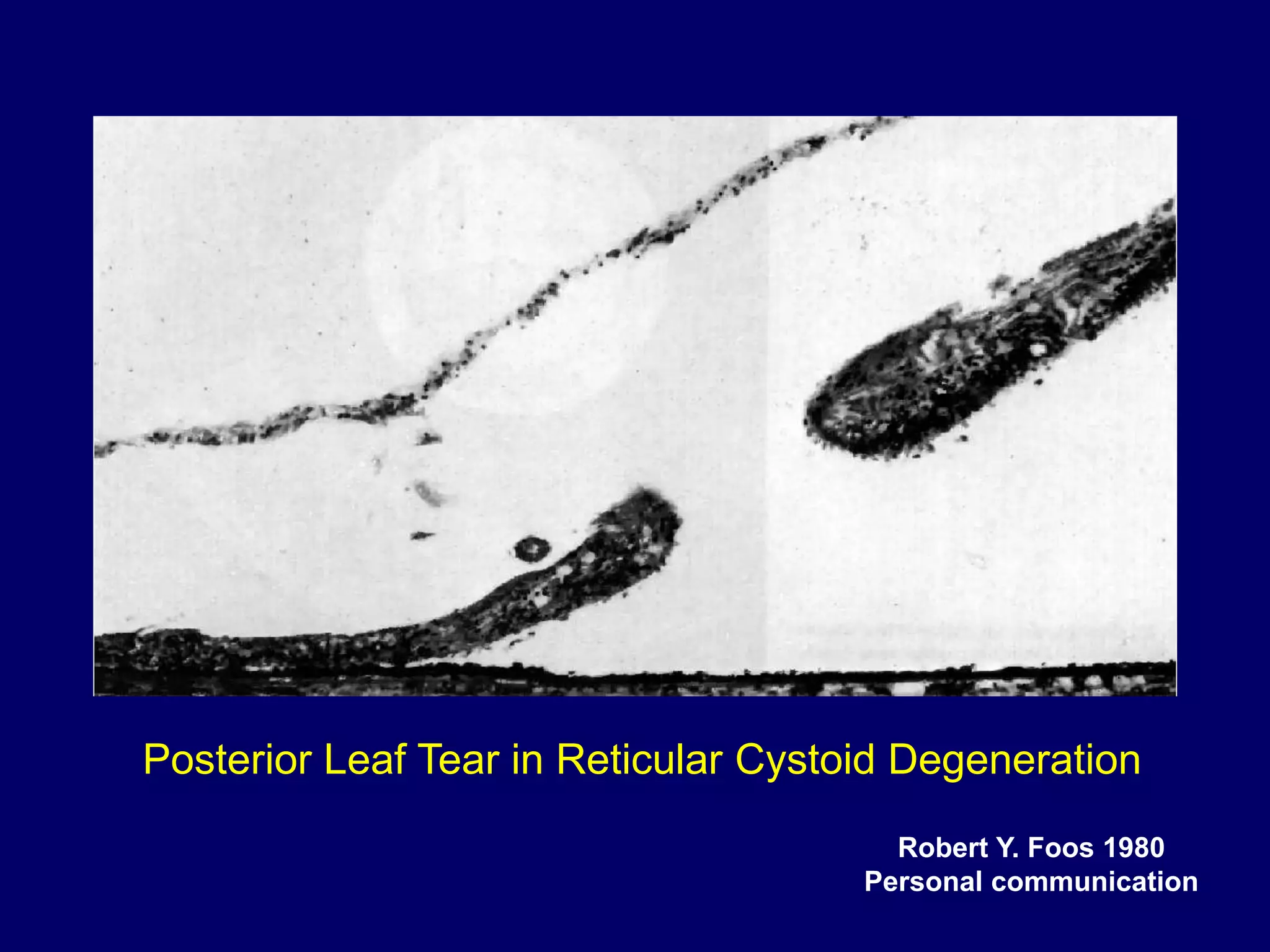















1. The document discusses different types of retinoschisis and retinal detachment, including sex-linked juvenile retinoschisis, degenerative retinoschisis, and retinal detachment associated with retinoschisis. 2. It describes the clinical features and pathogenesis of different types of retinoschisis. Degenerative retinoschisis can be flat or bullous and the bullous type is more likely to lead to retinal detachment due to holes in the outer wall. 3. Management of retinal detachment complicating retinoschisis requires identifying breaks in both the anterior and posterior retinal layers, complete drainage of subretinal fluid, and often a broad buckle to support the schitic retina













































































