Peripheral retinal degenerationsare classified according to
the following criteria:
■ Location: equatorial, peripheral, or combined
■ Patho morphology: trophic, tractional, atrophic, or
combined
■ Depth of retinal changes: intraretinal, retinal,
vitreoretinal, or Chori retinal.
■ Risk for retinal detachment
■ Prognosis: progressive or stationary
3.
Intra-Retinal
Degenerations
• Senile retinoschisis
•white-without-
pressure
• white-with-pressure
• dark-without-
pressure
• peripheral cystoid
degeneration
• snowflake
degeneration
• pearl degeneration
Vitreoretinal
Degenerations
• lattice degeneration
• snail-track
degeneration
• retinal tufts
• peripheral retinal
breaks
Chori retinal
Degenerations
• paving-stone
degeneration
• peripheral retinal
drusen
the following are the commonly used classifications of peripheral retinal
degenerations based on the depth of retinal changes observed on optical
coherence tomography (OCT):
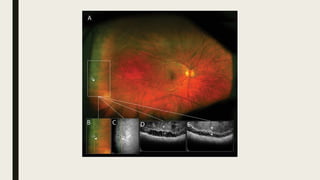
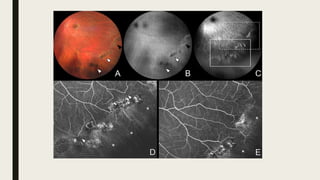
Senile Retinoschisis:
■ Definition:Splitting of layers of the neurosensory retina by thick fluid
■ Prevalence: Found in 2%–7% of the general population; more common in people aged ≥40
years and in hyperopic eyes
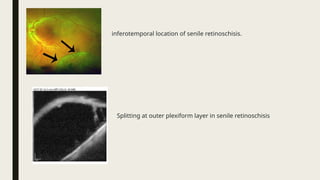
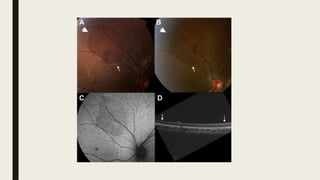
■ Characteristics: Lesion is a bullous elevation of the peripheral retina, most commonly in the
inferotemporal quadrant
■ Findings: Mostly asymptomatic
■ Immobile with movement of the eye; produces an absolute field defect
■ Complications: May involve posterior pole and lead to retinal detachment
■ Primary cause of retinal detachment in 0.05%–2.5% of cases
■ Diagnosis: OCT findings include intraretinal hyporreflective cavities with destruction and
thickening of the retinal pigment epithelium (RPE) and separation of the neurosensory retina
with splitting at the outer plexiform layer[1]
■ Treatment: Argon laser photocoagulation when patients are symptomatic or there is
progressive retinal detachment threatening the macula
6.
inferotemporal location ofsenile retinoschisis.
Splitting at outer plexiform layer in senile retinoschisis
7.
White-Without-Pressure
■ Definition: Distinctivewhite appearance of the peripheral retina without indentation and without mechanical
stimulus
■ Prevalence: Found in up to 30% of normal eyes; often bilateral; more frequently diagnosed in younger patients;
may be associated with longer axial length
■ Characteristics: Whiter than the retina in white with pressure; choroidal markings are almost obscured. Found
in the post-equatorial region at the base of the vitreous and ora serrata. Whiteness is further accentuated with
scleral depression. Margins are sharply demarcated from normal retina
– Can also appear as irregular, translucent areas in the retinal periphery with a red-brown border
– Lesions may have scalloped edges and may appear to move over time due to possible migratory nature[2]
■ The exact cause is unknown. One school of thought states it to be a manifestation of peripheral vitreous
traction while another believes it to be simply an abnormal reflex from a structurally normal vitreoretinal
interface
■ Frequently causes confusion with subclinical retinal detachment and retinoschisis, but indentation clearly
reveals that the retina is still apposed to the RPE
■ Diagnosis: OCT shows white areas corresponding to hyperreflective outer retinal layers and ellipsoid zone, with
no vitreous traction
– Fluorescein angiography may show patterns, including multiple pinpoint areas of hyperfluorescence and
increased peripheral fluorescence[2]
– Fundus autofluorescence may demonstrate relative hypofluorescence within lesions suggestive of
potentially reduced lipofuscin density in RPE cells[2]
■ Treatment: There is a low risk for association with retinal detachment, so patients are watched and examined
every 1–2 years
9.
White-With-Pressure
■ Definition: Distinctivemilky white or opalescent appearance of the peripheral retina
that is observed in many normal eyes when examined with scleral depression; term
used to describe flat peripheral detachment without any retinal break[3]
– Must be carefully distinguished from a subclinical peripheral retinal
detachment
■ Prevalence: Seen in around 30%–35% of eyes examined with scleral depression;
incidence increases with age; no sex predilection; more commonly observed in
myopic eyes during the second decade of life[3]
■ Findings: The retina appears normal without depression
– Inferonasal quadrant is the least likely to be affected
■ Complications: Benign condition; not associated with retinal breaks
11.
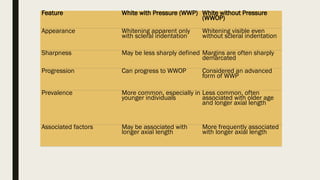
Feature White withPressure (WWP) White without Pressure
(WWOP)
Appearance Whitening apparent only
with scleral indentation
Whitening visible even
without scleral indentation
Sharpness May be less sharply defined Margins are often sharply
demarcated
Progression Can progress to WWOP Considered an advanced
form of WWP
Prevalence More common, especially in
younger individuals
Less common, often
associated with older age
and longer axial length
Associated factors May be associated with
longer axial length
More frequently associated
with longer axial length
12.
Dark-Without-Pressure
■ Definition: Flat,brown fundus lesion with well-defined margins in the equator of the
peripheral retina
■ Findings: Can be found posterior to the area of white-without-pressure and may look
like a retinal tear, posterior to ora serrata
■ Symptoms: usually none
■ Diagnosis: OCT findings show hyporeflectivity of the ellipsoid zone; border
corresponds to the site where the ellipsoid zone faded or disappeared[4]
■ Treatment: Benign condition; follow the patient with routine examinations
14.
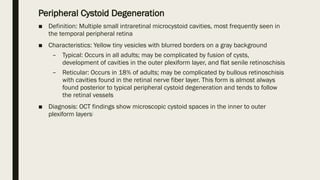
Peripheral Cystoid Degeneration
■Definition: Multiple small intraretinal microcystoid cavities, most frequently seen in
the temporal peripheral retina
■ Characteristics: Yellow tiny vesicles with blurred borders on a gray background
– Typical: Occurs in all adults; may be complicated by fusion of cysts,
development of cavities in the outer plexiform layer, and flat senile retinoschisis
– Reticular: Occurs in 18% of adults; may be complicated by bullous retinoschisis
with cavities found in the retinal nerve fiber layer. This form is almost always
found posterior to typical peripheral cystoid degeneration and tends to follow
the retinal vessels
■ Diagnosis: OCT findings show microscopic cystoid spaces in the inner to outer
plexiform layers[
16.
Snowflake Degeneration
■ Definition:Small yellowish dots in the peripheral retina that appear white due to light
reflection; small crystalline deposits in the retina from the ora serrata to the equator[2]
■ Prevalence: Rare
■ Findings: May span a wide band in more than one retinal quadrant, most often in the
superotemporal quadrant
– May be combined with other peripheral retinal degenerations (e.g. retinoschisis,
lattice, white-without pressure)
■ Complications: Retinal tears, retinal holes, and retinal detachment.
17.
Pearl Degeneration
■ Definition:Congenital retinal degeneration associated with white beads on the
retina
■ Prevalence: Found in up to 20% of patients
■ Characteristics: Ora pearls appear like drusen and are found either between the
RPE and Bruch’s membrane or floating above the RPE
■ Diagnosis: OCT findings show hyporeflective cavities with vitreous layers attached to
the top of the lesion
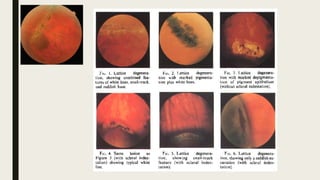
Lattice Degeneration.
■ Definition:Retinal thinning with loss of neurosensory layer; vitreoretinal adhesions at the
margin of lesion
■ Prevalence: Found in 6%–8% of patients
■ Characteristics: Retinal thinning with fibrosis and vitreous liquefaction over the lesion; spindle-
shaped areas of retinal thinning with or without pigmentation; arborizing white lines; frost-like
areas commonly located between the equator and the posterior border of the vitreous base[6]
– Typical: Well-outlined thinning with white crossing lines
– Atypical: Found adjacent to vessels in a radial pattern
■ Findings: Lesions have an oval or linear pattern; may be a single lesion or multiple lesions; may
have yellow deposits, pigment, atrophic holes, or retinal tears
■ Complications: Risk for retinal detachment and rhegmatogenous retinal detachment due to
vitreous traction
– Retinal detachment seen in 14%–35% of cases
■ Treatment: Prophylactic laser treatment is recommended in patients with vitreous traction and
retinal tears associated with flashes and floaters
23.
Snail-Track Degeneration
■ Definition:Groups of glistening white dots (which have been compared to frost
granules or salt); may be an early stage of lattice degeneration
■ Prevalence: Found in 10% of the general population; more commonly seen in
myopic eyes (40%)
■ Characteristics: Retinal thinning with vitreous liquefaction above the lesion;
associated vitreoretinal tractions
■ Findings: More often seen in the superotemporal and superonasal quadrants
■ Histologically, this lesion consists of degeneration of the neural elements of the
retina, leading to an atrophy of the tissues with lipid deposits in the internal retinal
layers
■ Complications: May lead to retinal tears in up to 54% of patients; retinal holes may
also be seen
■ Diagnosis: OCT findings show irregular retinal surface, vitreous destruction, and
vitreoretinal adhesions with traction at the margins
25.
Retinal Tufts
■ Definition:Area of retinal degeneration caused by attachment to and pulling of the
vitreous
■ Types include cystic, noncystic, and zonular traction tufts
■ Prevalence: Noncystic tufts are present in up to 72% of adults, cystic tufts are present
in up to 5% of adults, and zonular traction tufts are present in up to 15% of adults
■ Complications: Vitreous traction can lead to retinal tears and retinal detachment
■ Treatment: Prophylactic laser treatment is not recommended by the majority of
physicians; routine follow-up examinations are preferred.
27.
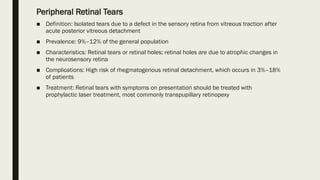
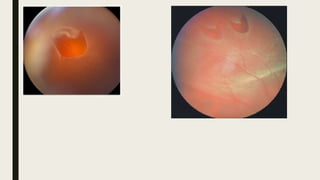
Peripheral Retinal Tears
■Definition: Isolated tears due to a defect in the sensory retina from vitreous traction after
acute posterior vitreous detachment
■ Prevalence: 9%–12% of the general population
■ Characteristics: Retinal tears or retinal holes; retinal holes are due to atrophic changes in
the neurosensory retina
■ Complications: High risk of rhegmatogenous retinal detachment, which occurs in 3%–18%
of patients
■ Treatment: Retinal tears with symptoms on presentation should be treated with
prophylactic laser treatment, most commonly transpupillary retinopexy
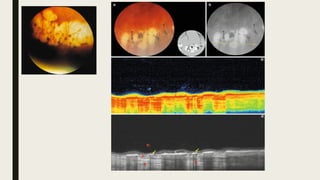
Paving-Stone Degeneration
■ Definition:Multiple rounded punched-out areas of choroidal and retinal atrophy
■ Prevalence: present in 4%–28% of patients; often bilateral; similar prevalence in
men and women; increasingly common with age
■ Characteristics: Lesions are yellow-white in color and may reveal underlying
choroidal vessels due to the sclera being partly visible through the atrophic choroid;
discrete margins that may be pigmented; may become confluent[7]
■ Findings: Located between the ora and equator with the size of one to several disc
diameters
■ More common in the inferonasal and temporal quadrants
■ Large choroidal vessels may be seen running through the base
■ Complications: Benign lesions not associated with complications
32.
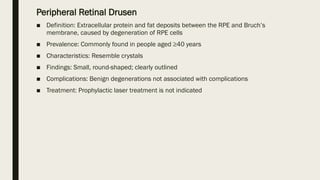
Peripheral Retinal Drusen
■Definition: Extracellular protein and fat deposits between the RPE and Bruch’s
membrane, caused by degeneration of RPE cells
■ Prevalence: Commonly found in people aged ≥40 years
■ Characteristics: Resemble crystals
■ Findings: Small, round-shaped; clearly outlined
■ Complications: Benign degenerations not associated with complications
■ Treatment: Prophylactic laser treatment is not indicated
34.
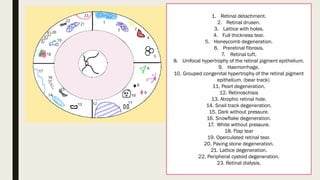
1. Retinal detachment.
2.Retinal drusen.
3. Lattice with holes.
4. Full thickness tear.
5. Honeycomb degeneration.
6. Preretinal fibrosis.
7. Retinal tuft.
8. Unifocal hypertrophy of the retinal pigment epithelium.
9. Haemorrhage.
10. Grouped congenital hypertrophy of the retinal pigment
epithelium. (bear track)
11. Pearl degeneration.
12. Retinoschisis
13. Atrophic retinal hole.
14. Snail track degeneration.
15. Dark without pressure.
16. Snowflake degeneration.
17. White without pressure.
18. Flap tear
19. Operculated retinal tear.
20. Paving stone degeneration.
21. Lattice degeneration.
22. Peripheral cystoid degeneration.
23. Retinal dialysis.

![Senile Retinoschisis:
■ Definition: Splitting of layers of the neurosensory retina by thick fluid
■ Prevalence: Found in 2%–7% of the general population; more common in people aged ≥40
years and in hyperopic eyes
■ Characteristics: Lesion is a bullous elevation of the peripheral retina, most commonly in the
inferotemporal quadrant
■ Findings: Mostly asymptomatic
■ Immobile with movement of the eye; produces an absolute field defect
■ Complications: May involve posterior pole and lead to retinal detachment
■ Primary cause of retinal detachment in 0.05%–2.5% of cases
■ Diagnosis: OCT findings include intraretinal hyporreflective cavities with destruction and
thickening of the retinal pigment epithelium (RPE) and separation of the neurosensory retina
with splitting at the outer plexiform layer[1]
■ Treatment: Argon laser photocoagulation when patients are symptomatic or there is
progressive retinal detachment threatening the macula](https://image.slidesharecdn.com/peripheralretinaldegenerations-250609112220-ee173786/85/Peripheral-Retinal-Degenerations-pptxxx-5-320.jpg)
![White-Without-Pressure
■ Definition: Distinctive white appearance of the peripheral retina without indentation and without mechanical
stimulus
■ Prevalence: Found in up to 30% of normal eyes; often bilateral; more frequently diagnosed in younger patients;
may be associated with longer axial length
■ Characteristics: Whiter than the retina in white with pressure; choroidal markings are almost obscured. Found
in the post-equatorial region at the base of the vitreous and ora serrata. Whiteness is further accentuated with
scleral depression. Margins are sharply demarcated from normal retina
– Can also appear as irregular, translucent areas in the retinal periphery with a red-brown border
– Lesions may have scalloped edges and may appear to move over time due to possible migratory nature[2]
■ The exact cause is unknown. One school of thought states it to be a manifestation of peripheral vitreous
traction while another believes it to be simply an abnormal reflex from a structurally normal vitreoretinal
interface
■ Frequently causes confusion with subclinical retinal detachment and retinoschisis, but indentation clearly
reveals that the retina is still apposed to the RPE
■ Diagnosis: OCT shows white areas corresponding to hyperreflective outer retinal layers and ellipsoid zone, with
no vitreous traction
– Fluorescein angiography may show patterns, including multiple pinpoint areas of hyperfluorescence and
increased peripheral fluorescence[2]
– Fundus autofluorescence may demonstrate relative hypofluorescence within lesions suggestive of
potentially reduced lipofuscin density in RPE cells[2]
■ Treatment: There is a low risk for association with retinal detachment, so patients are watched and examined
every 1–2 years](https://image.slidesharecdn.com/peripheralretinaldegenerations-250609112220-ee173786/85/Peripheral-Retinal-Degenerations-pptxxx-7-320.jpg)

![White-With-Pressure
■ Definition: Distinctive milky white or opalescent appearance of the peripheral retina
that is observed in many normal eyes when examined with scleral depression; term
used to describe flat peripheral detachment without any retinal break[3]
– Must be carefully distinguished from a subclinical peripheral retinal
detachment
■ Prevalence: Seen in around 30%–35% of eyes examined with scleral depression;
incidence increases with age; no sex predilection; more commonly observed in
myopic eyes during the second decade of life[3]
■ Findings: The retina appears normal without depression
– Inferonasal quadrant is the least likely to be affected
■ Complications: Benign condition; not associated with retinal breaks](https://image.slidesharecdn.com/peripheralretinaldegenerations-250609112220-ee173786/85/Peripheral-Retinal-Degenerations-pptxxx-9-320.jpg)

![Dark-Without-Pressure
■ Definition: Flat, brown fundus lesion with well-defined margins in the equator of the
peripheral retina
■ Findings: Can be found posterior to the area of white-without-pressure and may look
like a retinal tear, posterior to ora serrata
■ Symptoms: usually none
■ Diagnosis: OCT findings show hyporeflectivity of the ellipsoid zone; border
corresponds to the site where the ellipsoid zone faded or disappeared[4]
■ Treatment: Benign condition; follow the patient with routine examinations](https://image.slidesharecdn.com/peripheralretinaldegenerations-250609112220-ee173786/85/Peripheral-Retinal-Degenerations-pptxxx-12-320.jpg)
![Snowflake Degeneration
■ Definition: Small yellowish dots in the peripheral retina that appear white due to light
reflection; small crystalline deposits in the retina from the ora serrata to the equator[2]
■ Prevalence: Rare
■ Findings: May span a wide band in more than one retinal quadrant, most often in the
superotemporal quadrant
– May be combined with other peripheral retinal degenerations (e.g. retinoschisis,
lattice, white-without pressure)
■ Complications: Retinal tears, retinal holes, and retinal detachment.](https://image.slidesharecdn.com/peripheralretinaldegenerations-250609112220-ee173786/85/Peripheral-Retinal-Degenerations-pptxxx-16-320.jpg)
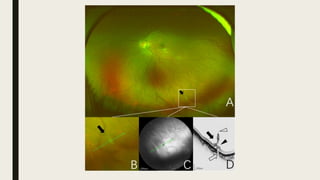
![Lattice Degeneration.
■ Definition: Retinal thinning with loss of neurosensory layer; vitreoretinal adhesions at the
margin of lesion
■ Prevalence: Found in 6%–8% of patients
■ Characteristics: Retinal thinning with fibrosis and vitreous liquefaction over the lesion; spindle-
shaped areas of retinal thinning with or without pigmentation; arborizing white lines; frost-like
areas commonly located between the equator and the posterior border of the vitreous base[6]
– Typical: Well-outlined thinning with white crossing lines
– Atypical: Found adjacent to vessels in a radial pattern
■ Findings: Lesions have an oval or linear pattern; may be a single lesion or multiple lesions; may
have yellow deposits, pigment, atrophic holes, or retinal tears
■ Complications: Risk for retinal detachment and rhegmatogenous retinal detachment due to
vitreous traction
– Retinal detachment seen in 14%–35% of cases
■ Treatment: Prophylactic laser treatment is recommended in patients with vitreous traction and
retinal tears associated with flashes and floaters](https://image.slidesharecdn.com/peripheralretinaldegenerations-250609112220-ee173786/85/Peripheral-Retinal-Degenerations-pptxxx-19-320.jpg)


![Paving-Stone Degeneration
■ Definition: Multiple rounded punched-out areas of choroidal and retinal atrophy
■ Prevalence: present in 4%–28% of patients; often bilateral; similar prevalence in
men and women; increasingly common with age
■ Characteristics: Lesions are yellow-white in color and may reveal underlying
choroidal vessels due to the sclera being partly visible through the atrophic choroid;
discrete margins that may be pigmented; may become confluent[7]
■ Findings: Located between the ora and equator with the size of one to several disc
diameters
■ More common in the inferonasal and temporal quadrants
■ Large choroidal vessels may be seen running through the base
■ Complications: Benign lesions not associated with complications](https://image.slidesharecdn.com/peripheralretinaldegenerations-250609112220-ee173786/85/Peripheral-Retinal-Degenerations-pptxxx-30-320.jpg)


















































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)















