Downloaded 925 times

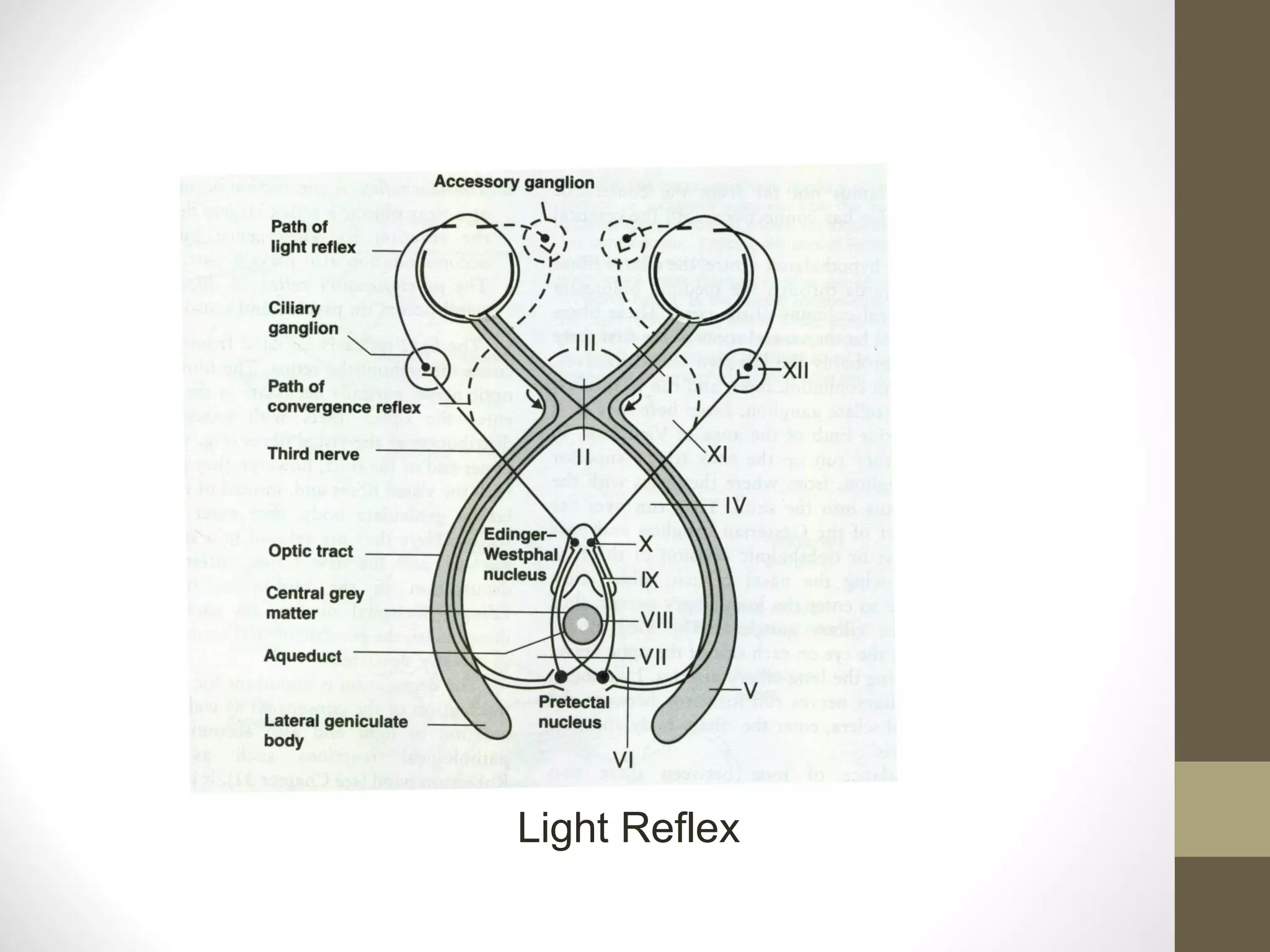






















The document discusses normal and abnormal pupillary reflexes. It describes the anatomy and physiology behind the light reflex and near reflex. The light reflex involves transmission of signals from the retina through the optic pathway to the Edinger-Westphal nucleus which controls the iris sphincter and dilator muscles. The near reflex involves a triad of accommodation, convergence, and pupillary constriction. It also discusses various pupil abnormalities that can occur due to lesions in the afferent or efferent pathways as well as pharmacologic agents that cause miosis or mydriasis. Specific conditions mentioned include Horner's syndrome, Adie's tonic pupil, and Argyll Robertson pupil.























































































