Downloaded 342 times


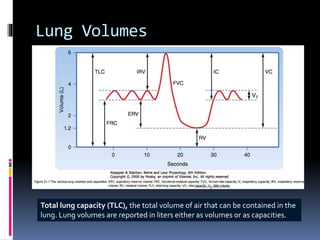
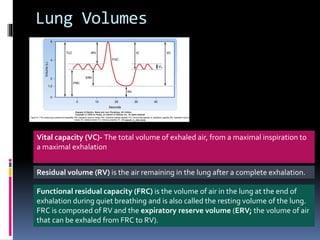
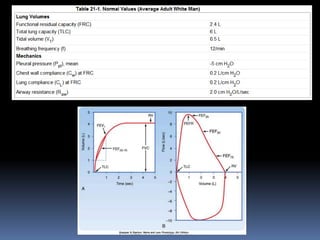
![Lung Volumes
(tidal volume [VT]) that is moved with each quiet breath is measured.](https://image.slidesharecdn.com/respifunctionalanatomy-150310095311-conversion-gate01/85/Respi-functional-anatomy-58-320.jpg)



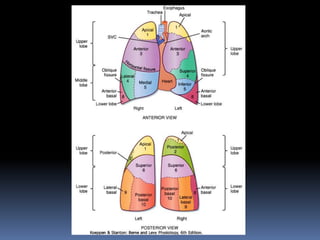
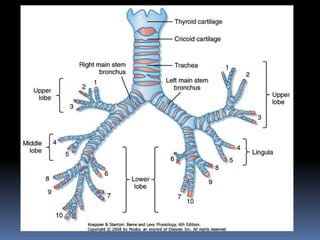
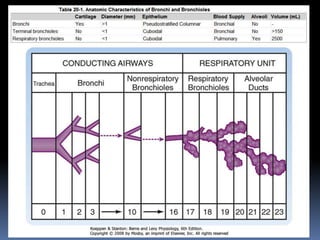
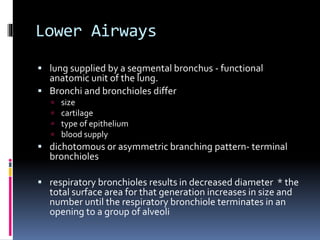
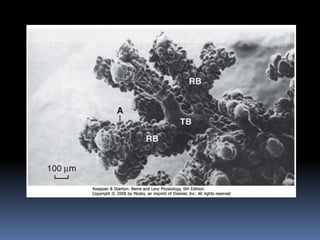
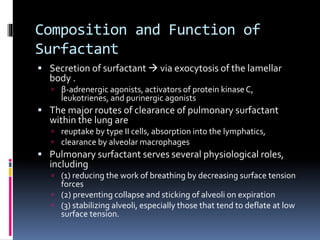
This document discusses the anatomy and physiology of the respiratory system. It describes the structure and function of the upper airways including the nose, sinuses, and larynx. It then covers the lower airways including the trachea, bronchi, bronchioles, and respiratory units containing the alveoli. It also discusses gas exchange, blood supply, innervation, and control of respiration.