




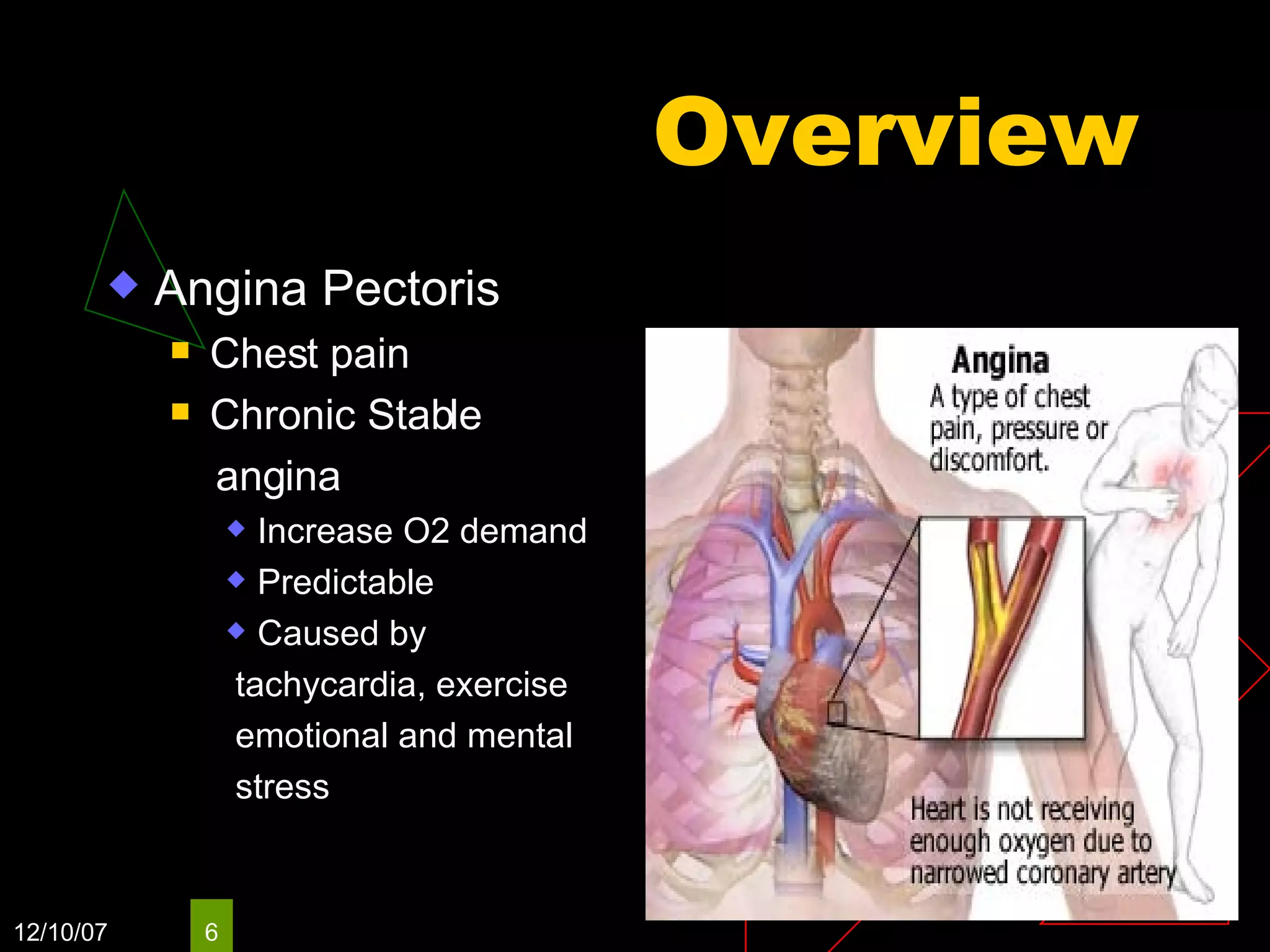



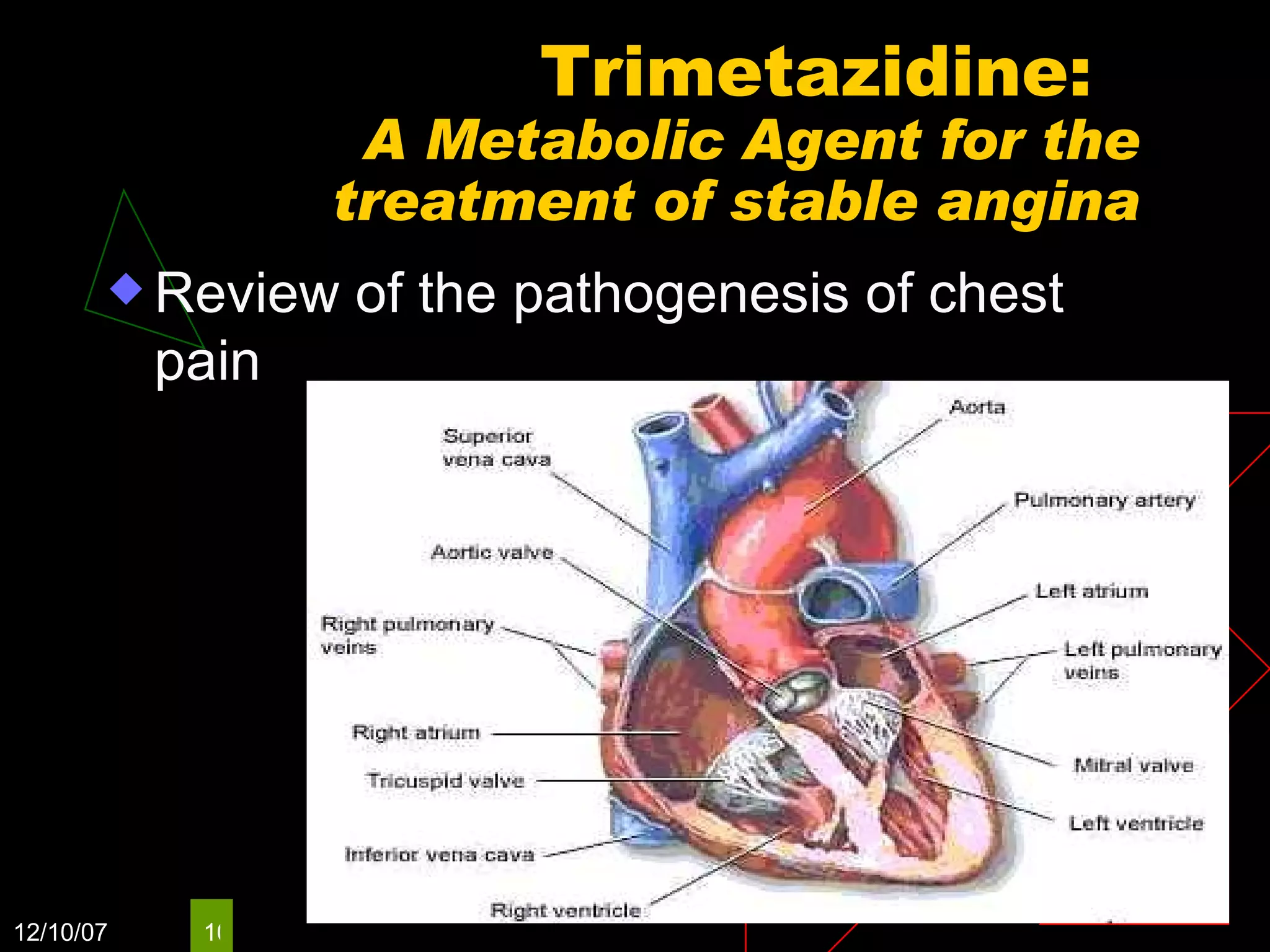























This document discusses treatment options for chronic stable angina, including the metabolic agent trimetazidine. It provides an overview of angina and its epidemiology. Trimetazidine improves energy metabolism in ischemic heart tissue by inhibiting fatty acid oxidation and stimulating glucose utilization. Clinical trials show trimetazidine reduces angina symptoms and improves exercise tolerance. It may benefit patients with heart failure or diabetes by optimizing energy production and preserving heart cell function.






























































![7. Ischaemic Heart Disease and Acute Coronary Syndromes [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/7-251128082316-c3f9588b-thumbnail.jpg?width=640&height=640&fit=bounds)










































