The document discusses respiratory physiology, including:
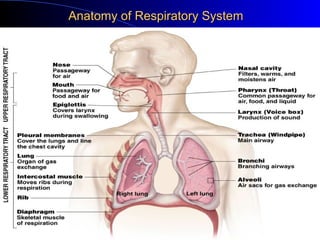
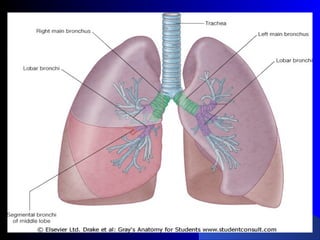
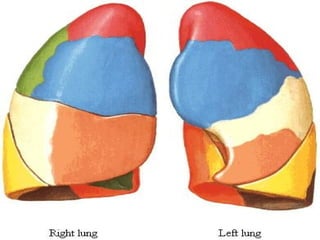
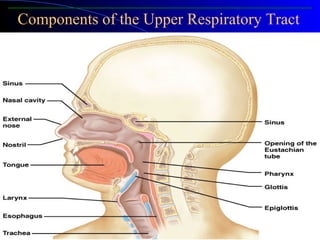
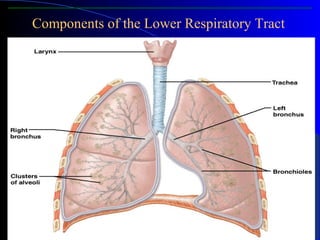
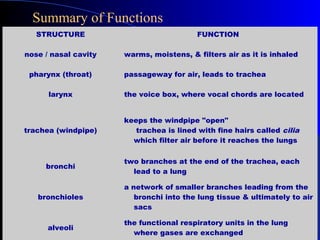
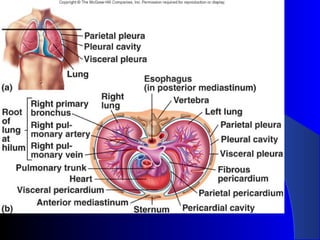
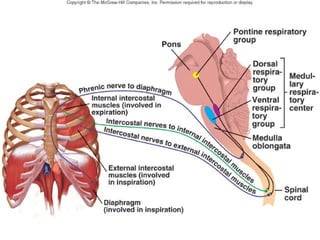
1) The anatomy of the respiratory system including the upper and lower respiratory tract.
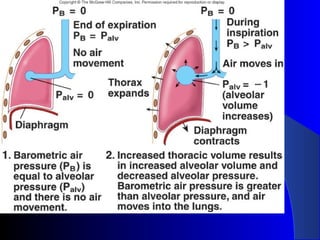
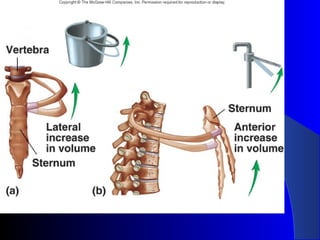
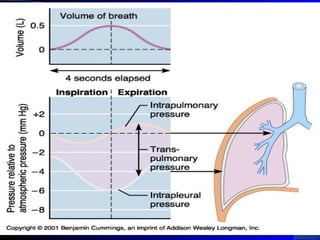
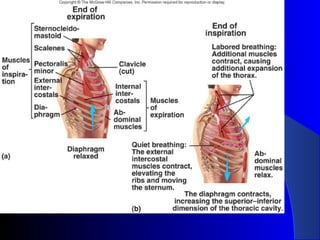
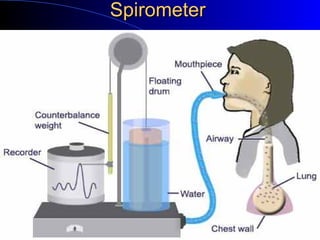
2) Pulmonary ventilation driven by pressure differences caused by contraction of respiratory muscles.
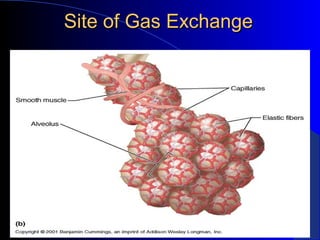
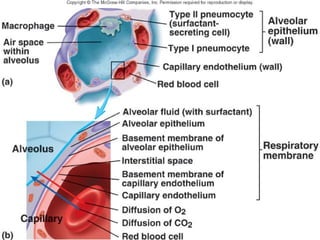
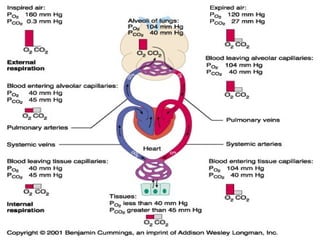
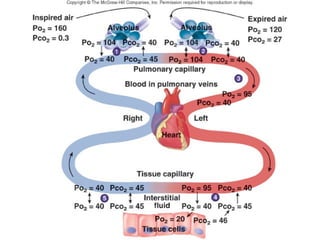
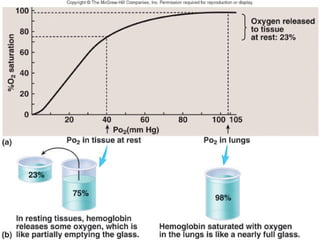
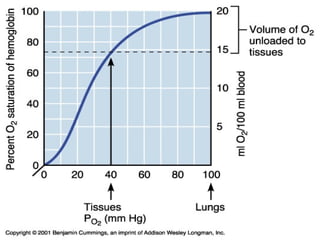
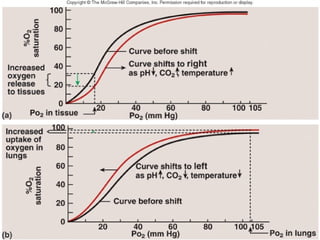
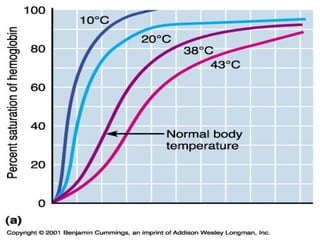
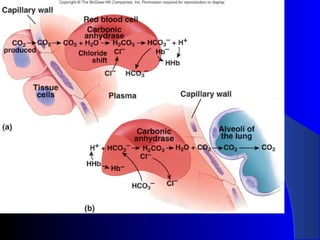
3) Gas exchange that occurs via diffusion between alveoli and capillaries in the lungs. Oxygen binds to hemoglobin while carbon dioxide is transported as bicarbonate.
4) Controls of respiration centered in the medulla that regulate rate and depth of breathing in response to changes in oxygen and carbon dioxide levels.