Downloaded 1,151 times
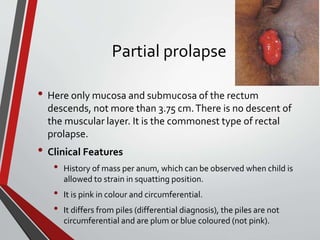
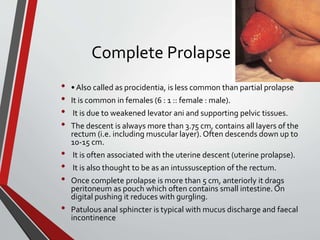
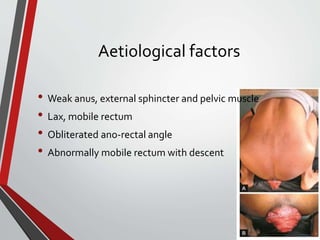
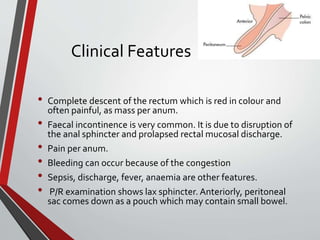
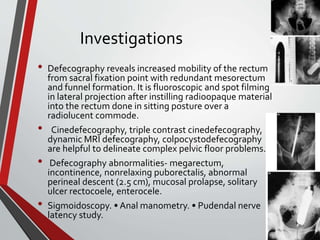



This document discusses rectal prolapse, which is the protrusion of the rectum outside of the body. It describes the types of rectal prolapse as partial or complete. Risk factors include weakened muscles, trauma from childbirth, and conditions that increase abdominal pressure. Treatment depends on the type and severity of prolapse, ranging from injections to repair surgery via abdominal or perineal approaches. Complications of surgery include nerve damage, infection, and recurrence of prolapse.