Downloaded 1,127 times



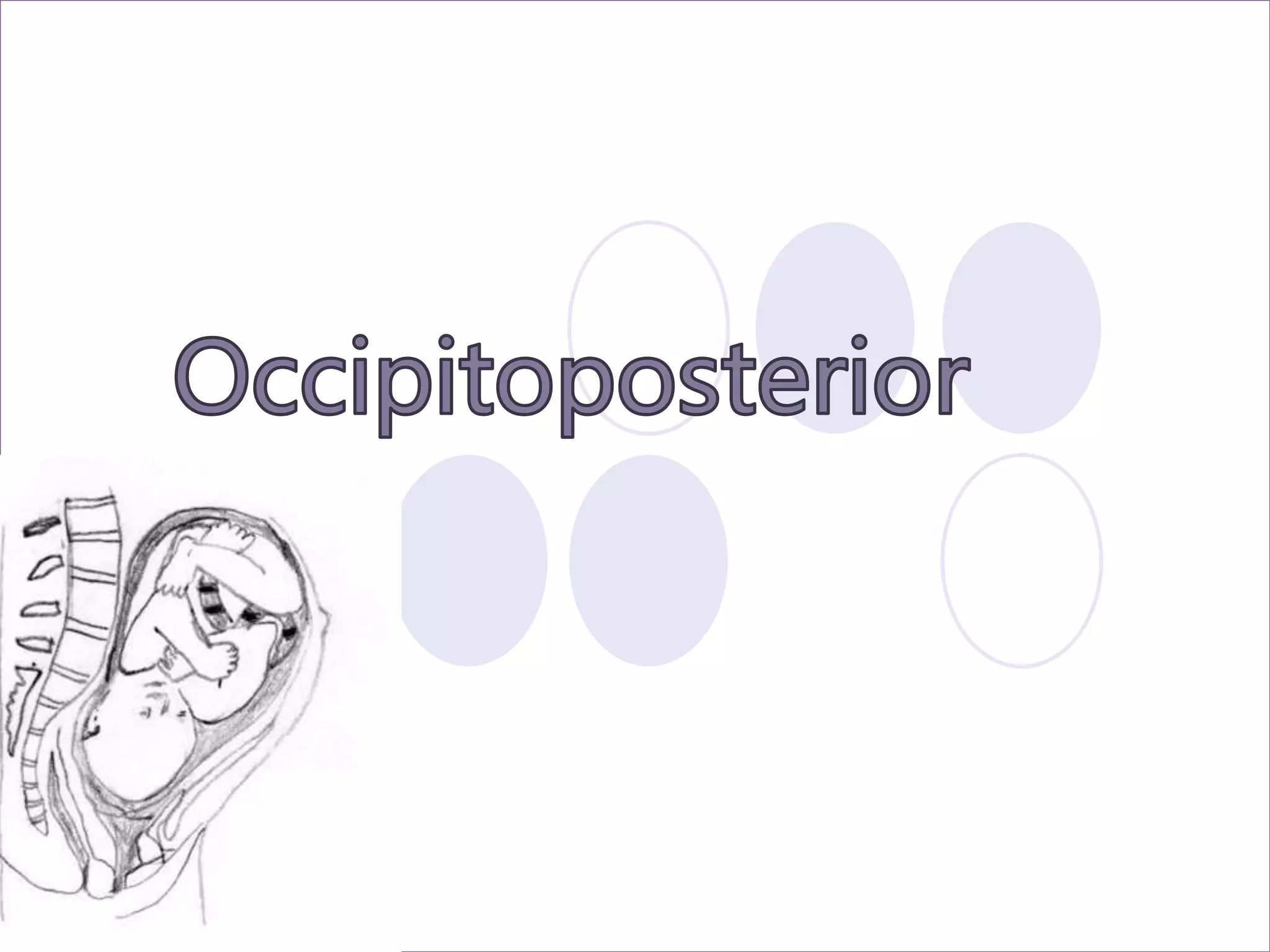








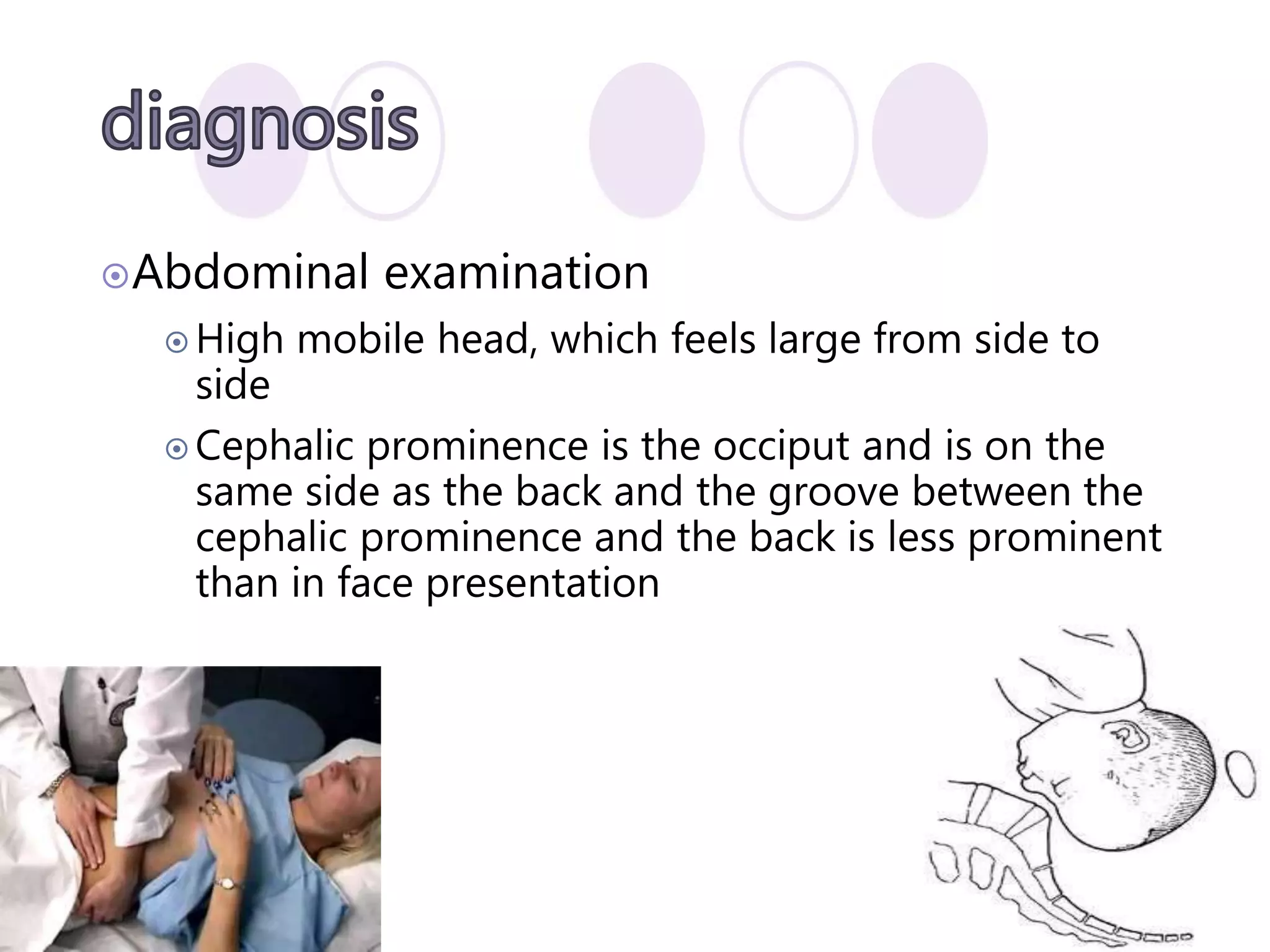







This document discusses fetal positioning and presentations during labor and delivery. It begins by defining non-vertex presentations including breech, face, brow, transverse, and compound. It then discusses the causes of non-vertex presentations and describes the different positions including occiput posterior. The document provides details on assessing various positions through abdominal and vaginal exams. It concludes by outlining the management of different non-vertex positions, including allowing natural rotation, augmentation of labor, operative vaginal delivery, or caesarean section if needed.

































































































