Downloaded 244 times








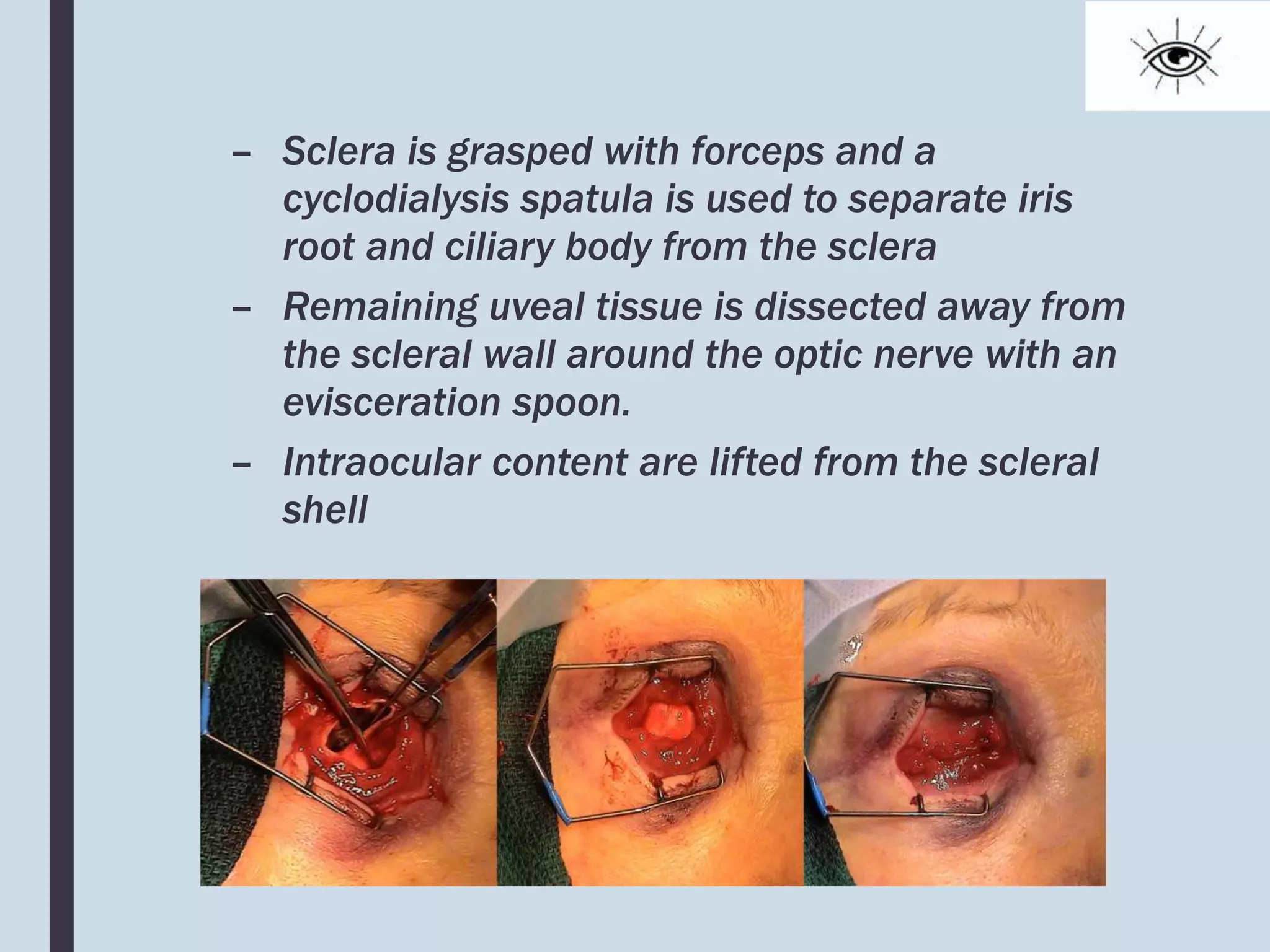





The document outlines the definitions, indications, surgical techniques, and potential complications related to enucleation and evisceration, both procedures for eye removal. Enucleation involves the complete removal of the eyeball, while evisceration removes the internal contents, leaving the scleral shell. It emphasizes the importance of pre-operative ultrasound to rule out malignancy and provides detailed surgical steps along with associated risks.




























![EYE REMOVAL TECHNIQUES [FINAL COPY BY FAITH KIMELI.] (1).pptx](https://cdn.slidesharecdn.com/ss_thumbnails/eyeremovaltechniquesfinalcopybyfaithkimeli-250203210808-e559c479-thumbnail.jpg?width=640&height=640&fit=bounds)
















































