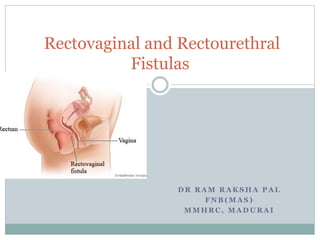
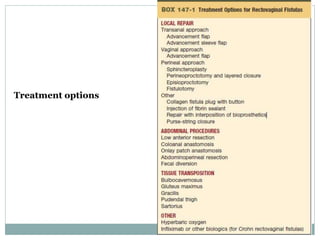
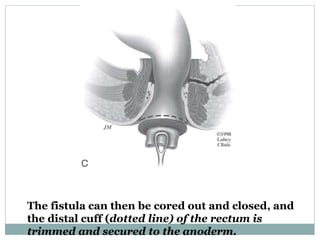
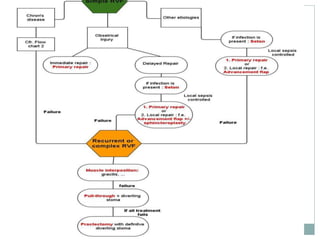
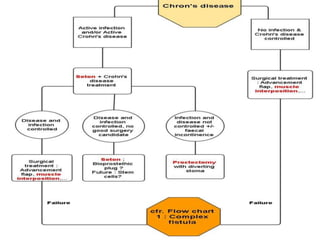
This document discusses rectovaginal and rectourethral fistulas. It begins by defining rectovaginal fistulas and discussing their causes, which include obstetric injuries, inflammatory bowel disease, prior surgery, and infections. It then covers the classification, presentation, examination, and diagnosis of rectovaginal fistulas. The document discusses the treatment options for rectovaginal fistulas, including medical therapy, surgical options such as local repairs via transvaginal or transanal approaches, and abdominal repairs. It provides details on techniques for local repairs like sliding flap repairs and transperineal repairs.