
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Dr Anisha Rectal prolapse.pptx
Similar to Dr Anisha Rectal prolapse.pptx (20)
Recently uploaded
Recently uploaded (20)
Dr Anisha Rectal prolapse.pptx
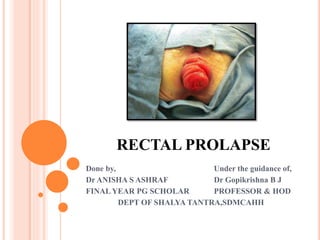
- 1. RECTAL PROLAPSE Done by, Under the guidance of, Dr ANISHA S ASHRAF Dr Gopikrishna B J FINAL YEAR PG SCHOLAR PROFESSOR & HOD DEPT OF SHALYA TANTRA,SDMCAHH
- 2. DEFINITION Protrusion of the rectal mucosa or full thickness of rectum through the anus is known as rectal prolapse. Circumferential descent of rectum through the anal canal
- 3. ETIOLOGY Sliding herniation of pouch of douglas through pelvic floor fascia into the anterior aspect of rectum Procidentia is a full thickness rectal intussusception starting approximately 7.5 cm above the dentate line which is extending beyond the anal verge. Commonly seen in infants, children and elderly Common in females 6:1
- 4. TYPES Partial Complete Hidden/ concealed PARTIAL RECTAL PROLAPSE
- 5. HIDDEN/CONCEALED PROLAPSE Internal intussusception of the sigmoid into the rectum or part of the rectum distally Do not come out of the anal orifice Only mucosa and submucosa separates from muscularis layer and descends May be associated with SRUS
- 6. PARTIAL PROLAPSE Only mucosa and submucosa comes out Length is not more than 3.75 cm Commonest type When the prolapsed mucosa is palpated between the finger and thumb, it is evident that it is composed of no more than a double layer of mucous membrane
- 7. IN INFANTS Sacral curve of rectum is not developed Direct downward course Diminished tone of anal musculature
- 8. IN CHILDREN Faulty bowel habit Straining – diarrheal attacks, whooping cough Malnutrition – loss of para-rectal fat Habitual constipation Associated with Fibrocystic disease, Neurological causes Mal development of the pelvis.
- 9. IN ADULTS Some loss of sphincter tone May be associated with 3rd degree haemorrhoids In female torn perineum - common in multipara Excessive straining in – BPH, Urethral strictures Excessive cough – Bronchitis Post operative cases – injury to sphincter muscles
- 10. CLINICAL FEATURES History of mass per anum Observed in squatting position Pink in color and circumferential (Haemorrhoids are not circumferential and plum or blue color)
- 11. MANAGEMENT Conservative: Treat malnutrition Digital reposition: By index finger after lubricating Appropriate bowel movements (Avoid constipation) – use of stool softeners and bulking agents rather than stimulant Avoid straining and adaptation of defecatory habit
- 12. SUBMUCOUS INJECTION 5% Phenol with Almond oil under GA – 10 ml in one sitting Only after digital reposition fails – 6 weeks Apex is injected circularly then reach submucosa Similarly base of the prolapse is injected Sterile inflammation – fibrosis – fixed to muscular coat Ethanolamine oleate can also be used
- 13. Alternatively 30 ml of tetracycline or oxytetracycline or hypertonic saline injection can also be used Initial injection is supported by Thiersch wiring – chromic catgut -(in 3 weeks)
- 14. APPLICATION OF BARRON BANDS Special rubber bands tied on the bases Endoscopically
- 15. OPERATIVE TREATMENT Thiersch’s operation: When conservative measures fail To patients of any age group Can be repeated if recurs In children with rectal prolapse, temporary wiring along with Goodsall’s ligature or injection sclerotherapy using thick catgut are often advocated
- 16. CONT... 2 midline small incisions one in front and one behind ½ inch away A long curved needle is passed from posterior incision emerging through anterior incision A piece of silver wire or stainless steel wire 20G is threaded through eye of the needle Polypropylene, Nylon can also be used
- 17. THIERSCH’S OPERATION CONT... Needle is taken out Reinsert needle from posterior opening Now taking out from other half through anterior incision with other end of wire Index finger (Little finger in children) should be inserted to anal cavity Assistant should twist the two ends of wire and make tight Twisted ends are cut short
- 18. THIERSCH’S OPERATION CONT... Anterior and posterior incisions are closed with stitches Gives mechanical support and chemical support by fibrous deposition around anal canal Wire can be removed after 3-12 months if required In children stitches should be removed to prevent stenosis (Strong chromic catgut can be used) Complication – wound – discharging sinus – Perianal sepsis; Anal stenosis; Breakdown of wire; fecal impaction; high recurrence;
- 19. EXCISION OF PROLAPSED MUCOSA Endoluminal stapling technique When a part of circumference is involved Base – ligated by Goodsall’s ligature Transfixed twice and tightened Redundant mucosa is excised If required cut margins are sutured interruptedly Can be adopted when associated with 3rd degree haemorrhoids
- 20. STAPLED TRANSANAL RECTAL RESECTION SURGERY (STARR) STARR – Exposure of the prolapse. b Traction sutures. c Opening of the prolapse. d Progressive stapling. e Control of hemostasis f Final appearance of the staple line
- 21. COMPLETE PROLAPSE (PROCIDENTIA) Prolapse of all layers of rectal wall It is descending sliding hernia Always more than 3.75 cm usually 10-15 cm Contains pouch of peritoneum anteriorly (If large may contain coils of intestine) Rare in children, common in elderly, women Due to weakened levator ani and supporting pelvic tissues
- 22. CLINICAL FEATURES Complete descent of rectum as mass per anum circumferentially - red in colour. Mass usually reducible and painless. Incarcerated or infected rectal prolapse is painful. May be associated with the uterine prolapse (uterine procidentia) in females. Faecal incontinence (75%) is very common – due to disruption of the anal sphincter and prolapsed rectal mucosal discharge. Bleeding – because of the congestion. Sepsis, discharge, fever, anaemia. P/R examination shows lax sphincter.
- 23. DIFFERENTIAL DIAGNOSIS Large 3rd degree haemorrhoids Large polypoid tumor Prolapse of sigmoid colon Intussusception Proctitis
- 24. ANORECTAL PHYSIOLOGICAL INVESTIGATION 1. ANORECTAL MANOMETRY: Normal resting pressure 40-80 mmHg – Function of internal anal sphincter Squeeze pressure – maximum voluntary contraction minus resting pressure. It is 40-80 mmHg above resting pressure. Reflects function of external anal sphincter Measured by placing water filled balloons attached to catheters and transducers placed in the anal canal
- 25. 2. NERVE CONDUCTION STUDIES To know about function of Pudendal nerve and branches: Pudendal nerve latency study: Specialized transducer attached to a glove like device is to be worn on the finger through which digital rectal examination is done Electrode in the finger is directed over the right and left levator ani complex to measure pudendal nerve terminal motor latency (PNTML) Normal : 1.8–2.2 msec. Prolonged in pudendal nerve damage
- 26. 3. DEFECOGRAPHY Increased mobility of rectum from sacral fixation point Fluoroscopic and spot filming in lateral projection after instilling radio-opaque material into the rectum Done in sitting posture over a radiolucent commode
- 27. 3. DEFECOGRAPHY CONT... For complex pelvic floor problems: Cinedefecography, triple contrast cinedefecography, dynamic MRI defecography, colpocystodefecography Preprolapse in defecography: Rectum is funnel shaped; lack of fixation to sacrum; excessive rectosigmoid mobility; Ring pocket formation; Intussusception Rectal prolapse in defecography: Redundant sigmoid colon, wide deep pouch of Douglas
- 28. DEFECOGRAPHIC GRADING OF RECTAL PROLAPSE N— normal rectal fixation and sphincter relaxation and rectal emptying 1—nonrelaxed puborectalis 2—mild intussusception 3—moderate intussusception 4—severe intussusception 5—prolapse R—rectocele
- 29. SIGMOIDOSCOPY To detect the tumor in the intussuscepted prolapsed rectum – Occasional
- 30. AIM OF MANAGEMENT To control the prolapse; to restore continence; to prevent constipation Should avoid abdominal repair in young males – may injure pelvic nerves – impotency Delorme’s operation is better option in young with complete prolapse Anal encircling surgeries using synthetic wires/mesh/suture materials are limited to extremely ill patients and elderly who will not withstand perineal proctectomy
- 31. MANAGEMENT PERINEAL PROCEDURES Delorme’s procedure Altemeier’s procedure Thiersch wiring ABDOMINAL PROCEDURES Wells operation – posterior rectopexy Ripstein sling operation – anterior rectopexy Mesh rectopexy Lahaut’s operation
- 32. FIXATION OPERATIONS 1. IVALON SPONGE WRAP OPERATION (WELLS’) Abdominal approach Rectum is fully mobilized posteriorly Rectangular sheet Ivalon sponge (Polyvinyl alcohol ) – sutured to the presacral fascia and periosteum of sacrum Mobilized rectum is drawn up Ivalon sponge is wrapped over and sutured Anterior surface is uncovered Ivalon sponge will initiate fibrosis and fixes rectum Chances of infection and fistula formation are high
- 33. 2. RECTOPEXY (LOCKHARDT MUMMERY OPERATION) Abdominal approach, rectum mobilization A curved incision about 2 inches in length is made midway between the anus and tip of coccyx Incision is deepened Fibers of external sphincter and anococcygeal ligament ligaments are cut Further fascia of Waldeyer is incised transversely Rectum is stripped off to 3rd sacral vertebra Resulting cavity is packed with long strips of guaze of polyvinyl alcohol sponge This is attached to fascia in front of the sacrum by 3 or 4 sutures
- 34. MESH RECTOPEXY Instead of Polyvinyl sponge, a marlex mesh is kept behind the rectum Sutured behind to sacrum then to the posterior and lateral surfaces Laparoscopic methods are popular – procedure of choice Constipation is one of the complications Some resect sigmoid colon with this procedure – Goldberg operation
- 35. LAPAROSCOPIC POSTERIOR MESH RECTOPEXY (LPMR) Ideal and good Prior bowel preparation is needed Head down, low lithotomy position Ports are placed Sigmoid colon is held by left side port Surgeon dissects from right side
- 36. Peritoneum on the right of the rectum is opened from sacral promontory downwards to reach presacral avascular plane Injury to autonomic nerves, ureters should be avoided Dissection is extended down for adequate mobilization Lateral ligaments are either divided or left alone Anterior mobilization along with Denonvillier’s fascia 5 cm below the peritoneal reflection
- 37. 10 x 6 cm polypropylene mesh is placed in the presacral space deep to rectum then fixed to presacral fascia along with sacrum and sacral promontory Mesh is sutured to rectal wall also on both sides using interrupted polypropylene sutures Only partial wrapping of mesh is done and peritoneum is closed using vicryl
- 38. 3. RECTAL SLING OPERATION (RIPSTEIN) Abdominal approach Rectum is mobilized down to the tip of the coccyx Rectum is freed from sacrum Rectum is pulled up taut 5 cm band of Teflon is placed around the rectum Free ends of band are sutured to Presacral fascia and periosteum of the sacrum 5 cm below the promontory of the sacrum Sling should be loose enough to allow one finger to pass between the Rectum and the sacrum
- 40. 4. PERINEAL APPROACH – DELORME’S OPERATION Mucosal sleeve resection and plication Prior bowel preparation Under Spinal anaesthesia in lithotomy position Collapsed rectum is pulled down as far as possible with Babcock’s forceps 1 in 2,00,000 adrenaline solution is injected into the submucosal plane of the rectum to cause haemostasis Longitudinal incision – with sharp scissor and cautery dissection
- 41. Mucosa is stripped off from the deeper muscular layer from 1 cm below the anal margin to the apex of the prolapsed rectum Series of chromic catgut sutures are placed to imbricate the underlying muscle – plication – by using vicryl 2-0 – interrupted suturing – all around – 12-15 stiches are needed After this rectal muscles are pulled up towards the anal canal Anal canal mucosa is sutured with rectal mucosa interrupted vicryl sutures Easy in elderly; relapse rates are high; does not correct defect
- 42. 5. LAHAUT’S OPERATION The whole of rectum and sigmoid colon are mobilized Held up Stitched with the rectus sheath Not popular nowadays
- 43. 6. GOLIGHER’S OPERATION Rectum is entirely mobilised up to anorectal ring Posterior muscular layer is fixed to pre- sacral fascia using interrupted polypropylene sutures
- 44. DEVADHAR RECTAL PLICATION Abdominal approach Junction between thicker lower part and thinner upper part of the intussusception is identified A purse string suture using silk is placed in front and laterally Further 3-4 interrupted submucosal Lambert sutures are placed to create reverse intussusception
- 45. RESECTION OPERATIONS 1.ANTERIOR RESECTION OF RECTUM: In lithotomy- trendelenberg position A guaze piece is inserted into the anus Long right paramedian incision from umbilicus to 2 cm below the pubic crest Inferior mesenteric artery is ligated Splenic flexure and descending colon are mobilized Rectum is pulled forward Separated from sacral promontory and presacral fascia as far down as the tip of the coccyx and pelvic floor muscle
- 46. Anteriorly seminal vesicles are pulled forward by using St. Mark’s retractor and dissection is done in between vesicles and rectum Denonvillier’s fascia is incised transversely till pelvic floor In female dissection is carried out between rectum and vagina Lateral ligaments are dissected Ligation of superior rectal arteries and veins
- 47. The proximal line of resection should be at convenient point at rectosigmoid junction or redundant sigmoid colon is also resected The anastomosis can be done to the anus by suturing or stapling Anastomosis is checked digitally or sigmoidoscopically Some fluid is placed in pelvis and air is blown from sigmoidoscope if no bubbles means anastomosis is satisfactory
- 48. The peritoneum is sutured to the pelvic colon well above the line of anastomosis A drain is placed in left iliac fossa into pre-sacral space Abdomen is closed in layers Drain is usually removed after 48 hours
- 49. 2. PERINEAL RECTOSIGMOIDECTOMY – ALTEMEIER’S PROCEDURE In Trendelenburg position or prone jack knife position Circular incision is made from the outer layer of the prolapse 2 cm proximal to the dentate line Anteriorly as the incision is deepened peritoneal cavity is opened Excision of the prolapsed rectum and associated sigmoid colon from below, and construction of a coloanal anastomosis.
- 51. SACRAL PROCEDURES In jack-knife position Incision is made over coccyx and para-sacral area Accessing pre-sacral and post-rectal space Rectum is mobilized and shortened by imbricating sutures Foreign material is placed in pre-sacral area None of these procedures has stood the test of time and become particularly popular
- 52. COMPLICATIONS OF RECTAL PROLAPSE Proctitis Ulceration Rarely bleeding Gangrene of the rectum Rarely anemia, sepsis and fever Rupture with evisceration
- 53. COMPLICATIONS OF SURGERY Injury to hypogastric nerve causing impotence Bladder dysfunction Bleeding from sacral venous plexus Injury to rectum and colon causing faecal fistula Constipation Recurrence of prolapse Improper correction of continence occurs in 50% cases Infection—proctitis/pelvic abscess, etc.
- 54. GUDA BHRAMSHA प्रवाहणातिसाराभ्ाां तिर्गच्छति र्ुदां बतहिः | रूक्षदुबगलदेहस्य िां र्ुदभ्रांशमातदशेि् ||६१|| su.ni. 13/63 The condition in which, the rectum protrudes due to the aggravation of Vayu in a weak and dry patient due to straining during defecation as in dysentery. In Charaka Samhita it has been described as complication Virechana Ativyapada In Astanga Hridaya, It has been named as Guda Nisarana
- 55. CHIKITSA र्ुदभ्रांशे र्ुदां स्विन्नां स्नेहाभ्क्तां प्रवेशयेि् | कारयेद्गोफणाबन्धां मध्यस्वच्छद्रेण चमगणा ||६१|| तवतिर्गमार्थं वायोश्च िेदयेच्च मुहुरमुगहुरिः | क्षीरे महत्पञ्चमूलां मूतिकाां चान्त्रवतजिगिाम् ||६२|| पक्त्वा िस्विि् पचेत्तैलां वािघ्नौिधसांयुिम् | र्ुदभ्रांशतमदां क ृ च्छ रां पािाभ्ङ्गाि् प्रसाधयेि् ||६३|| su.chi.20
- 56. The protruded part should be lubricated with Sneha and fomented then gently reintroduced manually The region of anus should then be bandaged in the manner of Gophana Bandha with an opening (Lying immediately below the anus), so not to interfere with emission of Vayu The affected part should then be constantly fomented Changeryadi Ghritapana
- 57. Mushikadi Taila: A quantity of milk, Mahapanchamula, and the flesh of the mouse, devoid of its intestines should be first boiled together along with Taila and Vataghna Dravyas Thus oil prepared by this method is used internally as well as externally to treat the difficult cases of Gudabhramsa
- 58. KSHARA KARMA IN GUDA BHRAMSHA
- 61. BEFORE KSHARA KARMA AFTER KSHARA KARMA (squatting position) AFTER KSHARA KARMA (Lithotomy position)
- 62. CONCLUSION Kshara application induces aseptic fibrosis of the anal mucosa and adheres it properly. During the wound healing process it causes cicatrisation and strengthens the anorectal ring. There will be no mass per rectum observed after Kshara application.