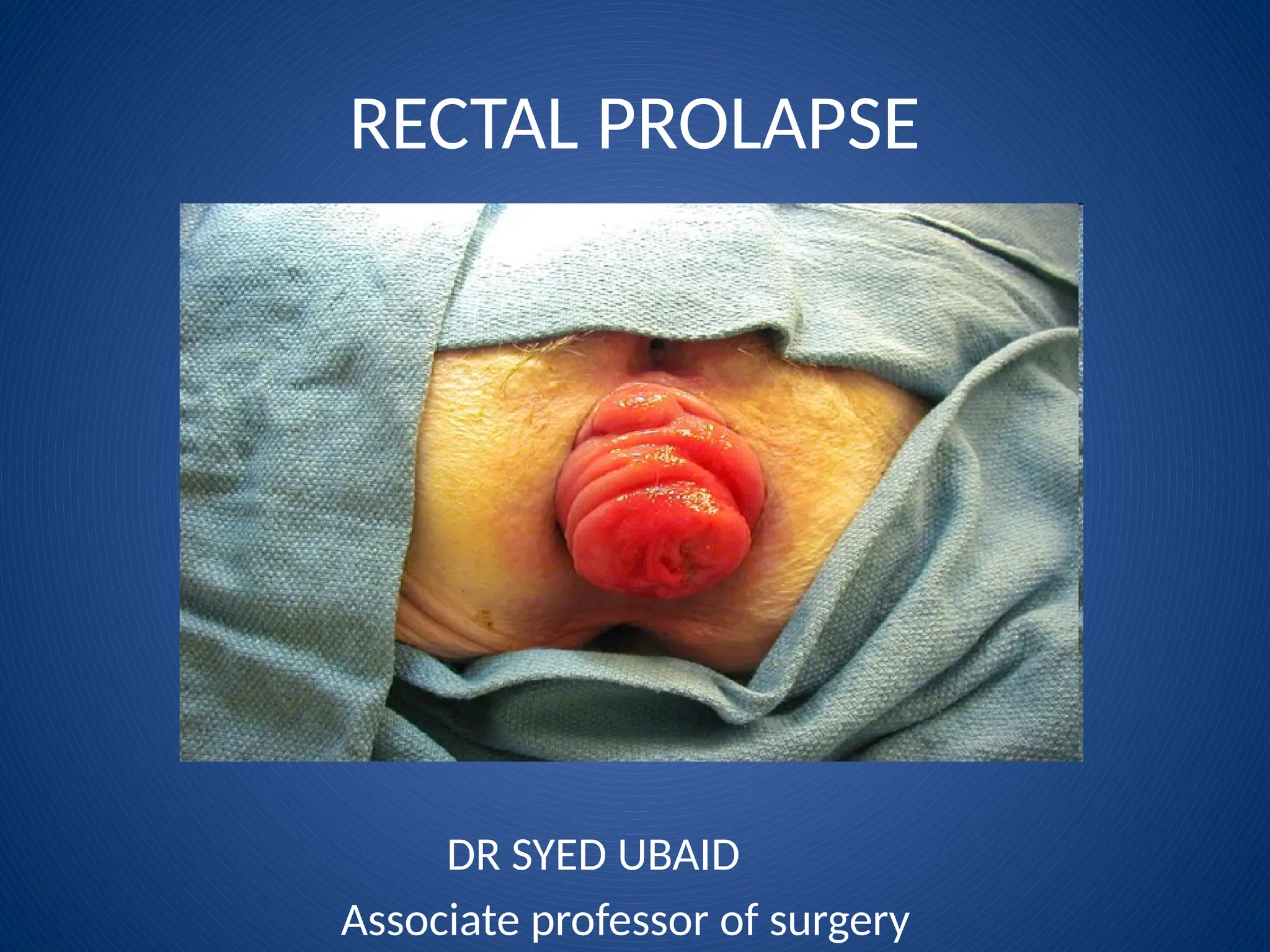
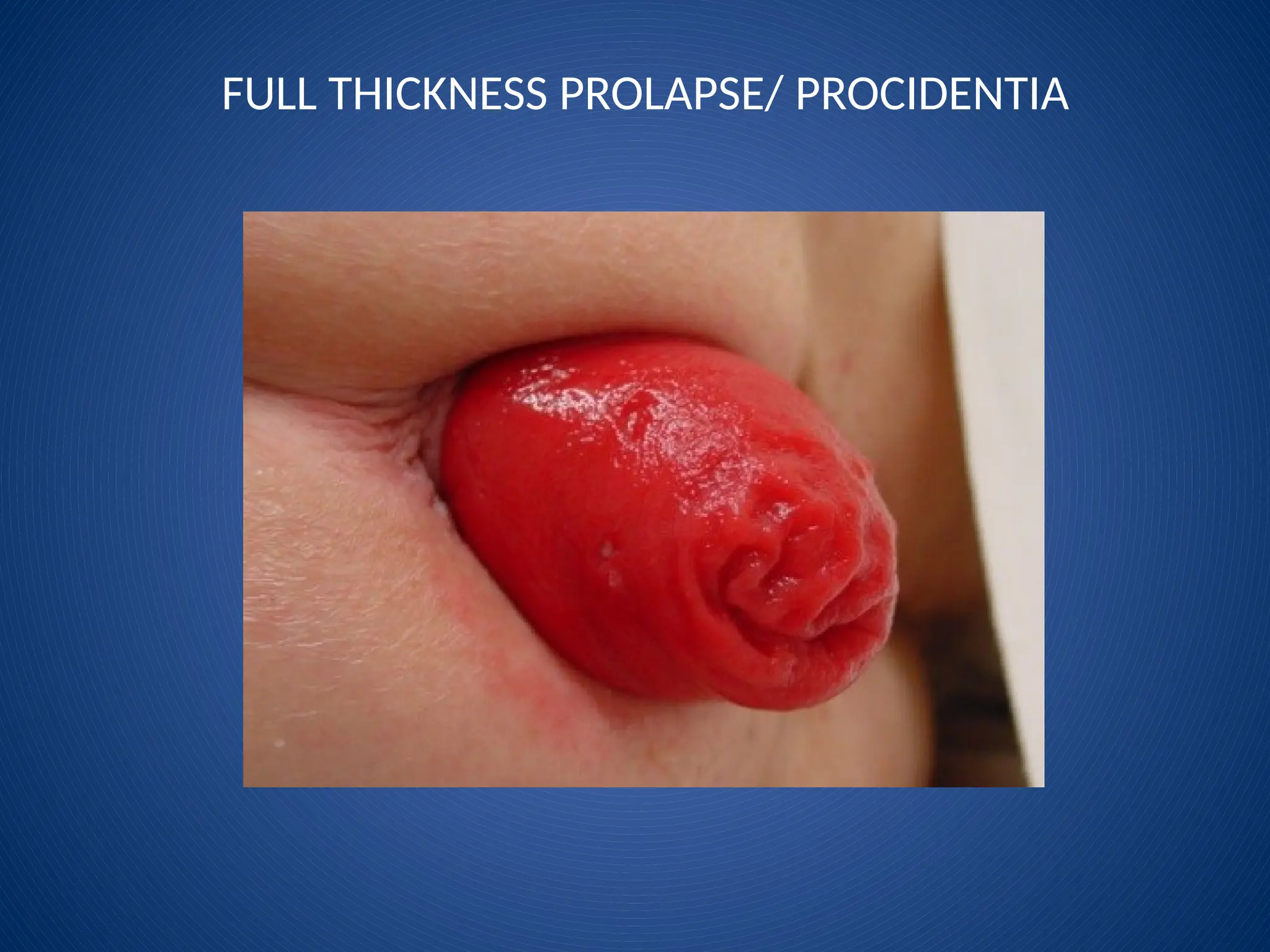
FULL THICKNESS PROLAPSE/PROCIDENTIA
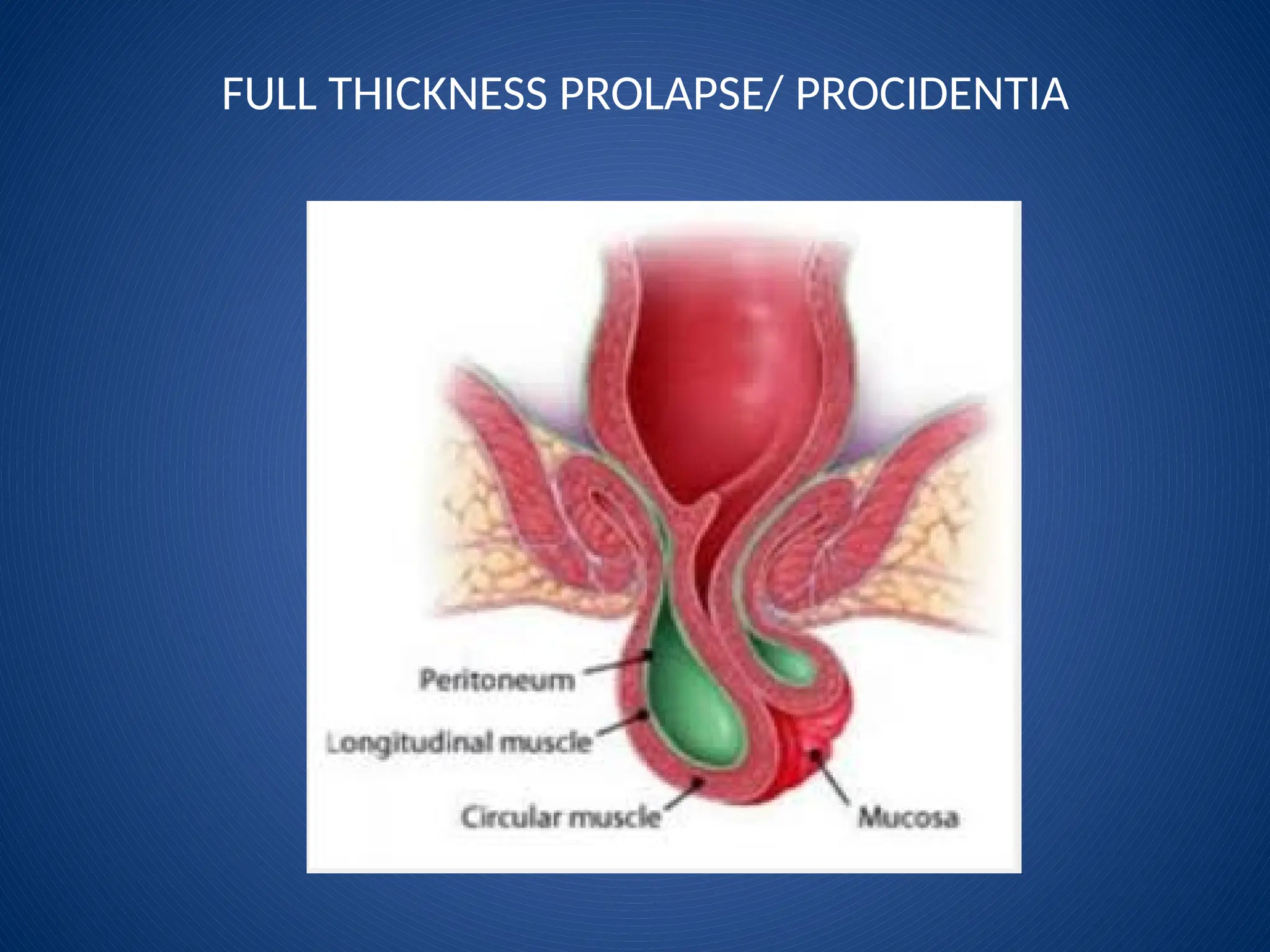
Full-thickness protrusion of the rectum through the anal
sphincters
● Protrussion consists of all layers of rectal wall
● 4-15 cm in length
● More common in females. Female to male ratio 6:1
● Commonly associated with prolapse of uterus
● A “falling down” of the rectum so that it’s out of the body
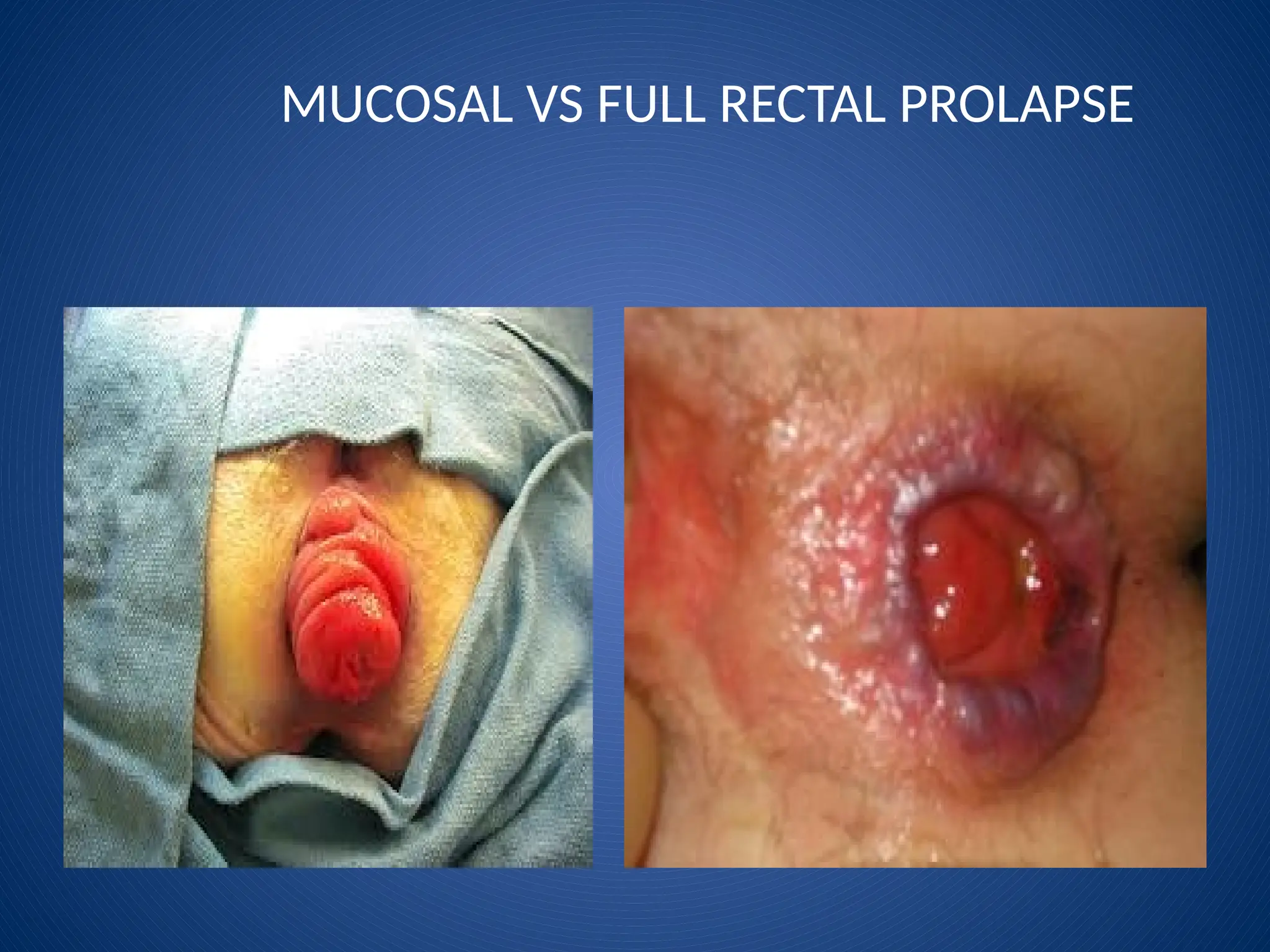
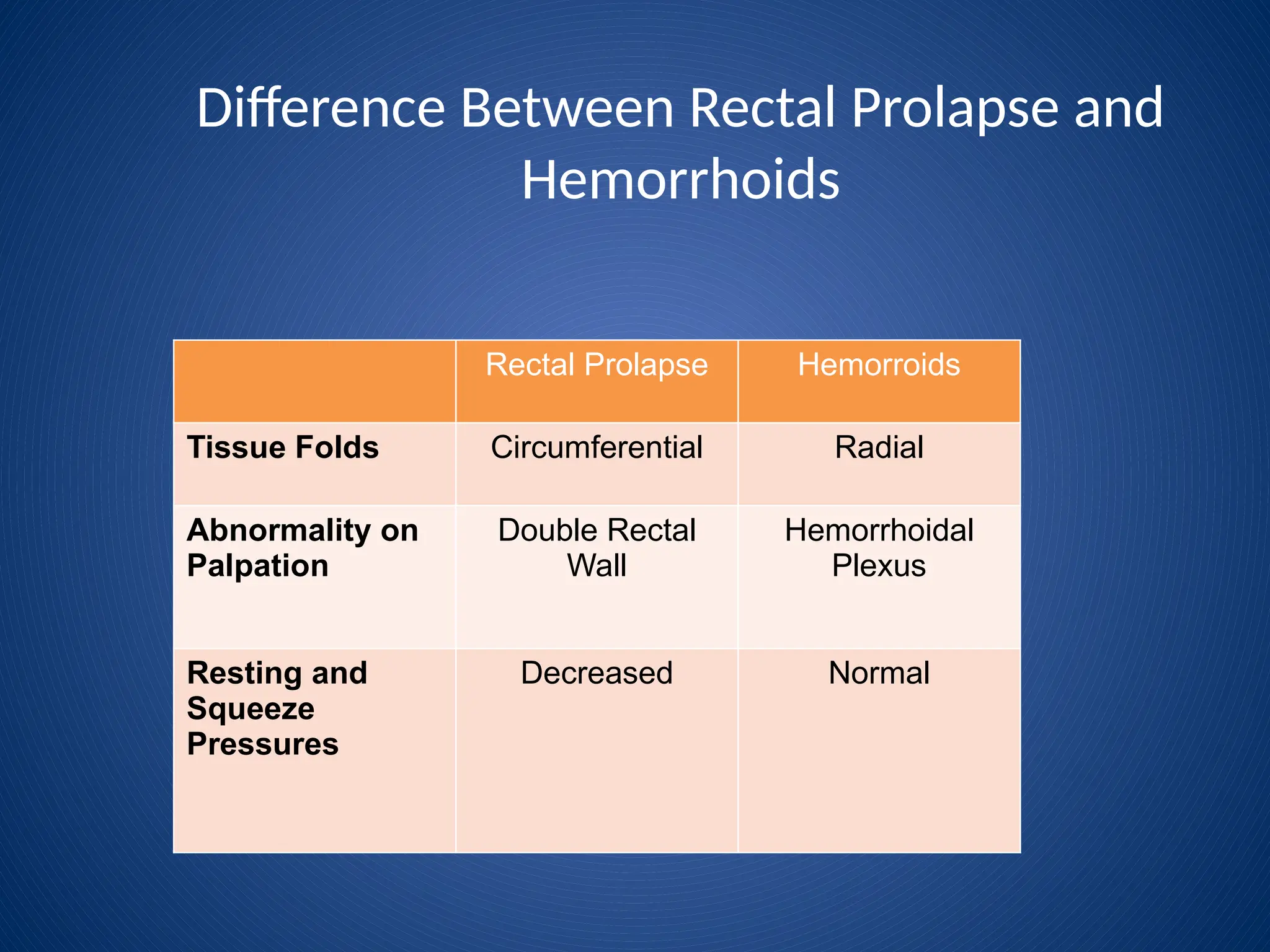
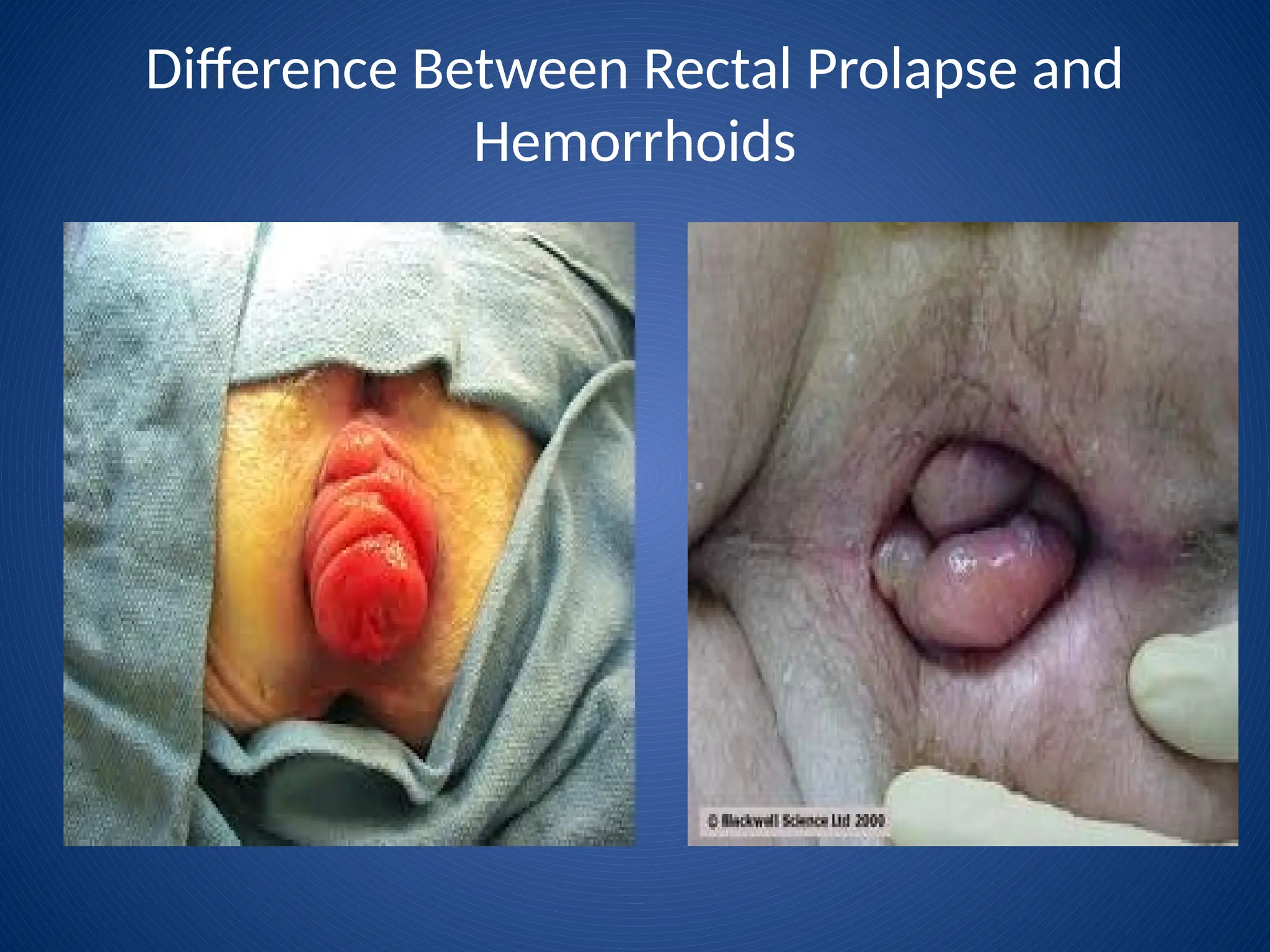
Rectal prolapse canbe distinguished from
prolapsed incarcerated internal hemorroids
by the characteristic concentric folds of
rectal prolapse and by the painless reduction
if not incarcerated.
14.
PATHOPHYSIOLOGY
• INFANTS
• Undevelopedsacral curve
• CHILDREN
• Attack of diarrhoea
• ADULTS
– Constipation (component of colonic dysmotility)
– Weakening/malfunctioning of pelvic floor/sphincters
– spastic pelvic floor
– Pudendal neuropathy (obstetric injuries, aging)
– Sphincter dysfunction (trauma, aging)
15.
Clinical Features
♦ MucusDischarge
♦ Rectal Bleeding
♦ Soilage
♦ Feeling of incomplete evacuation
♦ Diarrhea
♦ Itching
16.
Clinical Features
♦ Children:first three years (male=female)
● Cystic fibrosis, malnutrition, diarrhea, severe cough,
parasites
♦ Adults: majority are eldery female
● Females >50 – 6 times more likely than males
● 2/3 are multiparous
● Mental illness (depression, autism)
● Neurologic disorder
● Connective tissue disorder
● Constipation and straining
17.
Clinical Features
♦ Constipationis associated with prolapse in 30%-70% of pts
♦ Chronic straining, sensation of anorectal blockage, need of digital
evacation
♦ 60% have coexisting incontinence
● Stretching of anal sphincters
● Impaired rectal compliance
♦ 20-35% have associated urinary incontinence
18.
NON OPERATIVE MANAGMENT
•Treat constipation
• Fiber supplements
• Stool softeners
• Digital repositioning in infants and young children
• Sub mucosal injection of 5% phenol in almond oil
• Reduce incarcerated rectal prolapse
• Table sugar
19.
Surgical Treatment
♦ Mainstayin treatment of rectal prolapse
♦ Over 100 procedures
♦ In infants and young children rectum is sutured to sacrum in prone jack-
knife position.
♦ In adults with unilateral prolapse, redundant mucosa is excised or, if
circumferential, an endoluminal stapling technique can be used.
Full thickness prolapse:
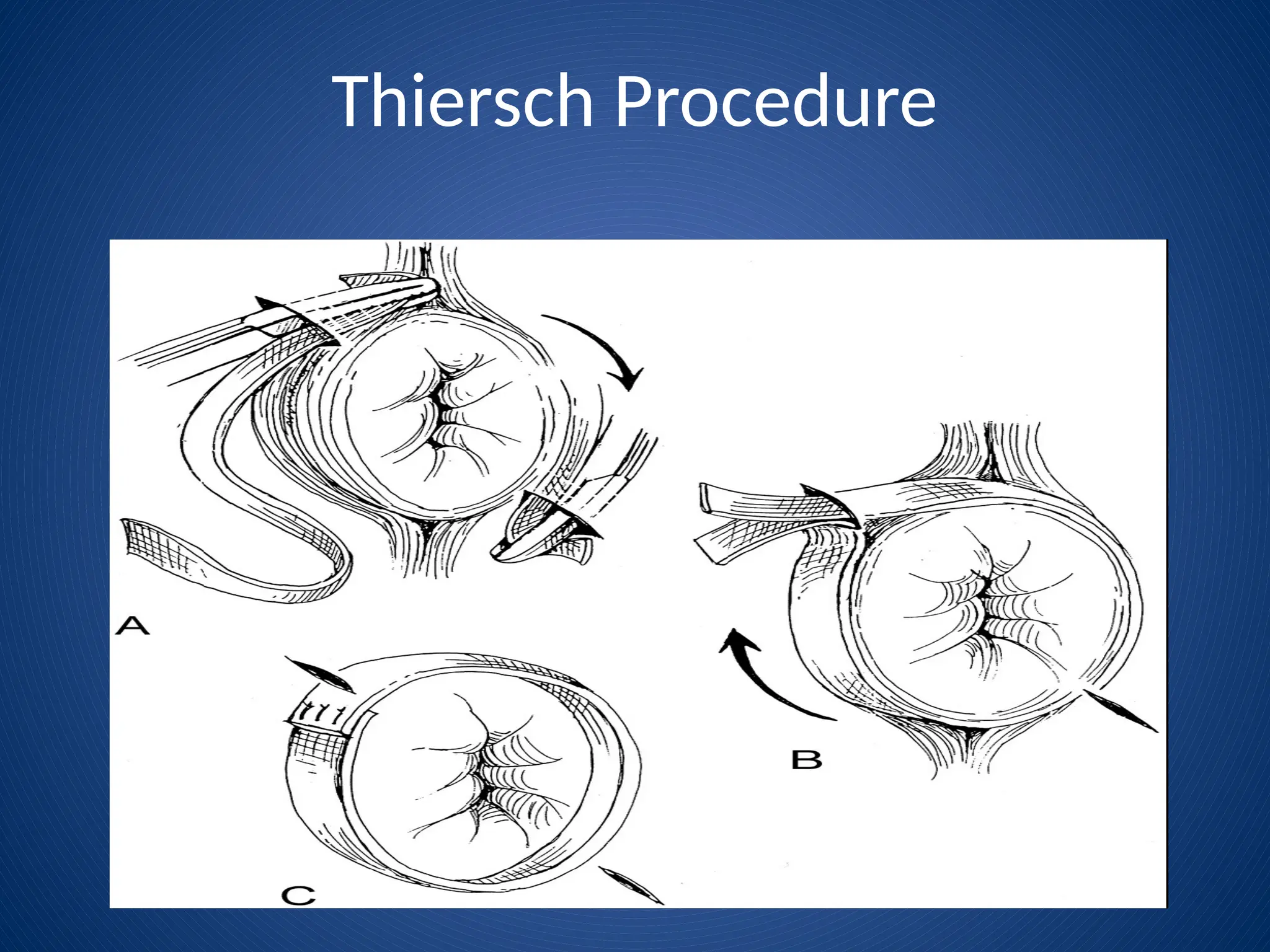
♦ Perineal procedures
● Resection, reefing, and encirclement
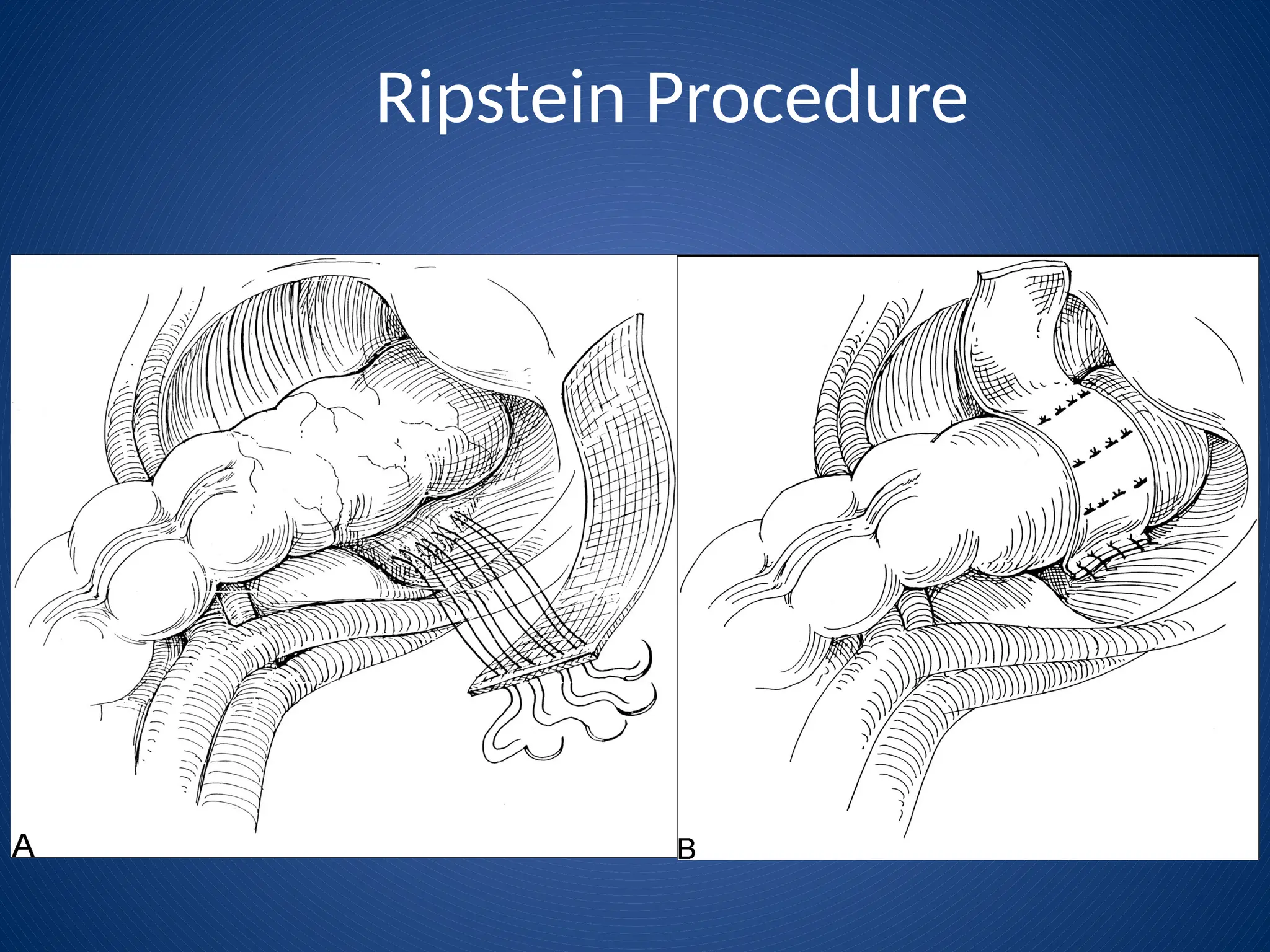
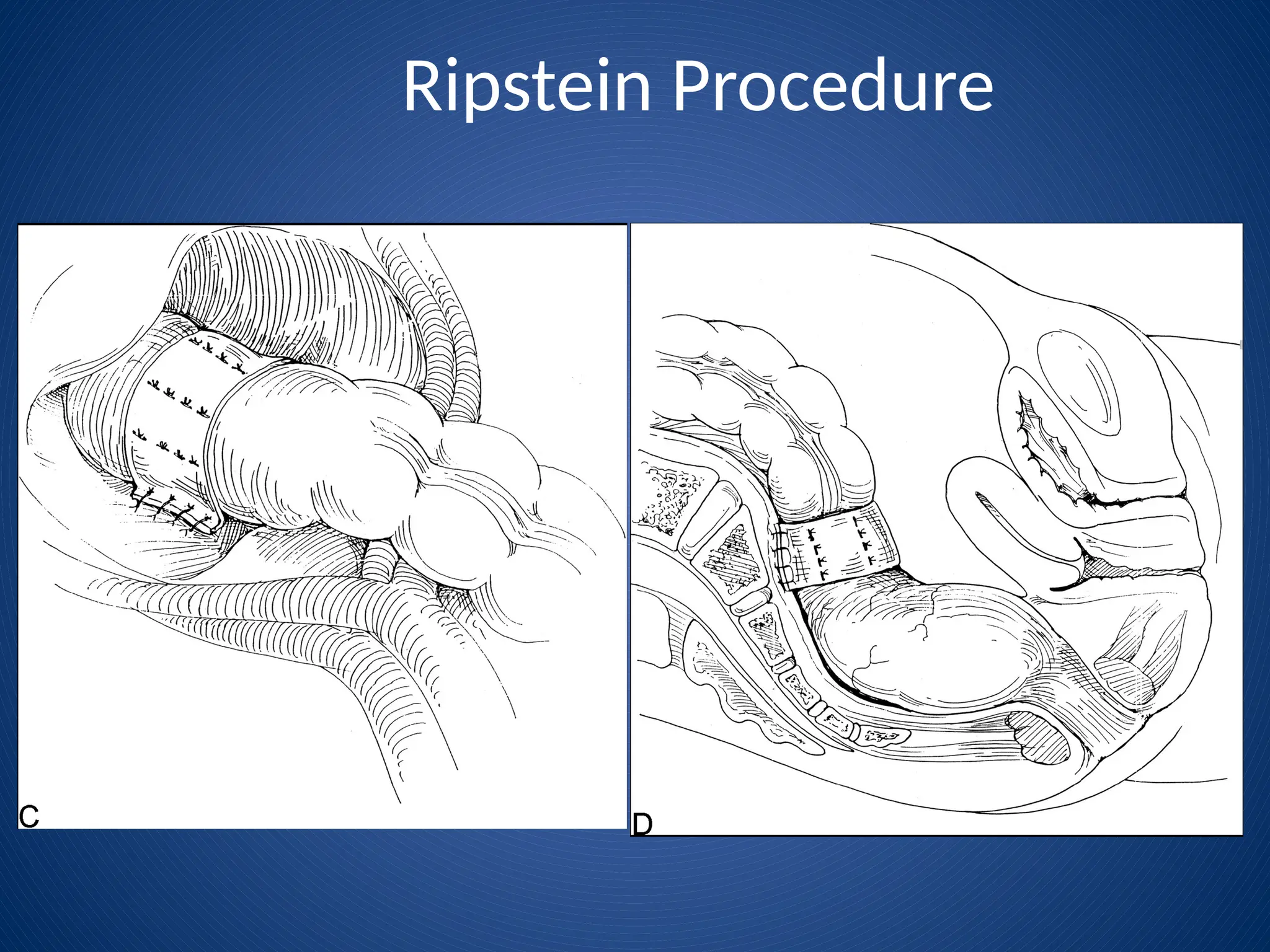
♦ Abdominal procedures
● Fixation, colon resection or combination of both
20.
Choosing Type ofSurgery
♦ Abdominal
● Recurrence low (<10%)
● ↑ constipation 50%
● Higher M & M esp.
with anastomosis
● Mesh placement –
stricture, migration,
erosion, infection
♦ Perineal
● Recurrence (20%)
● Constipation rate
unchanged
● Persistent incontinence
worse rate due to removal
of rectal resevoir
● Correction of associated
abnormalities (rectoceole,
sphincter)
● No pelvic dissection –
preserves sexual function
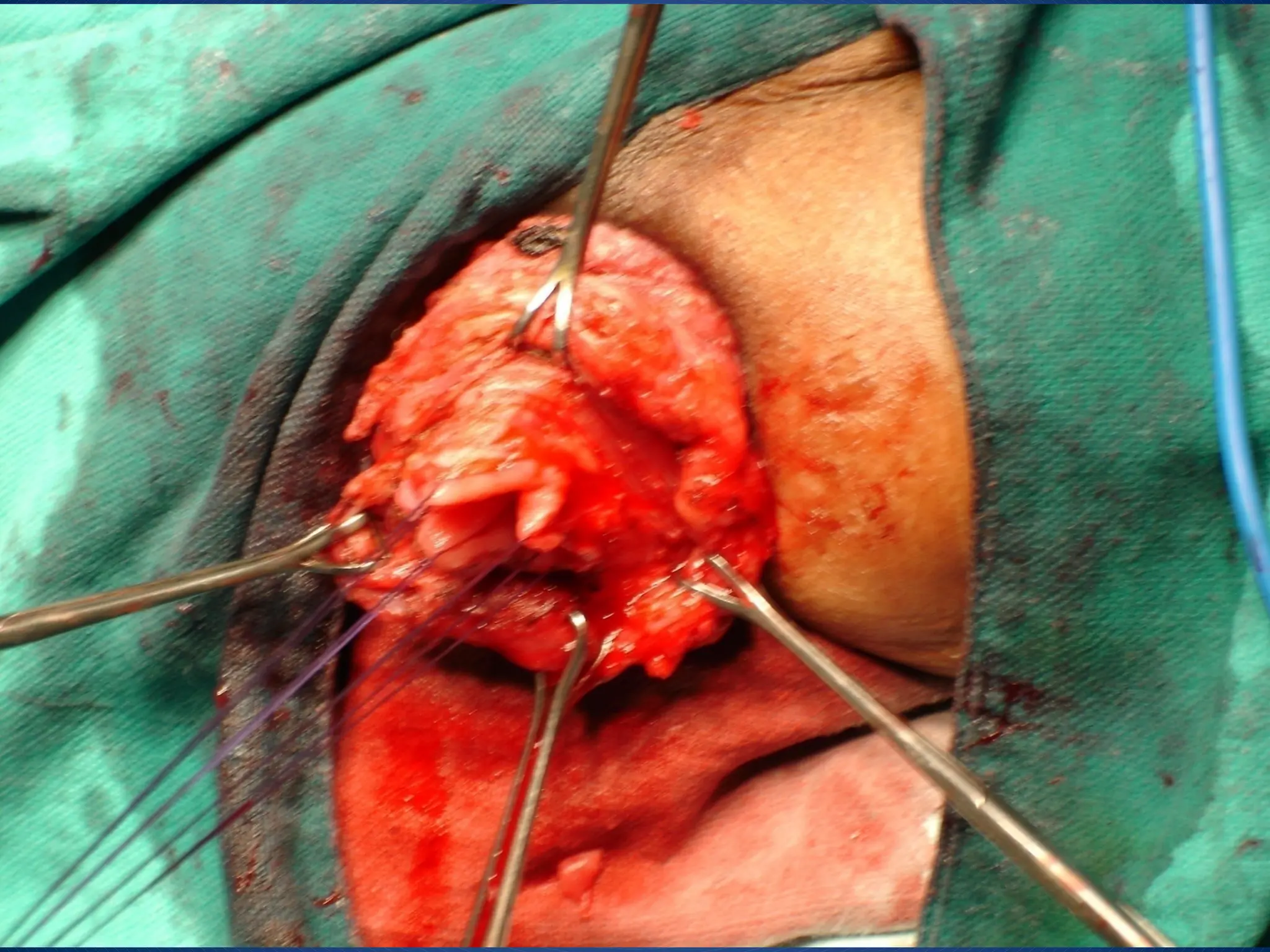
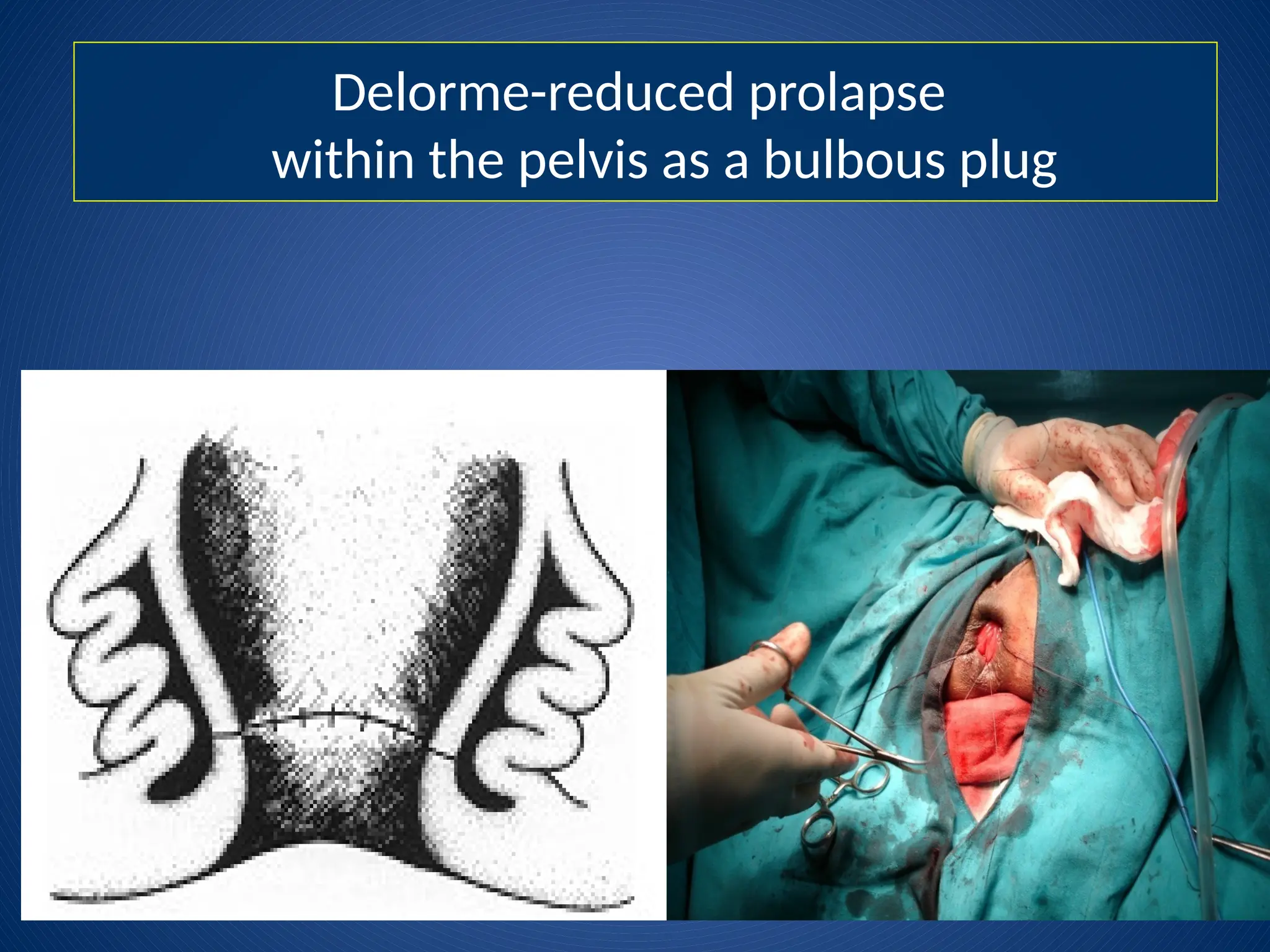
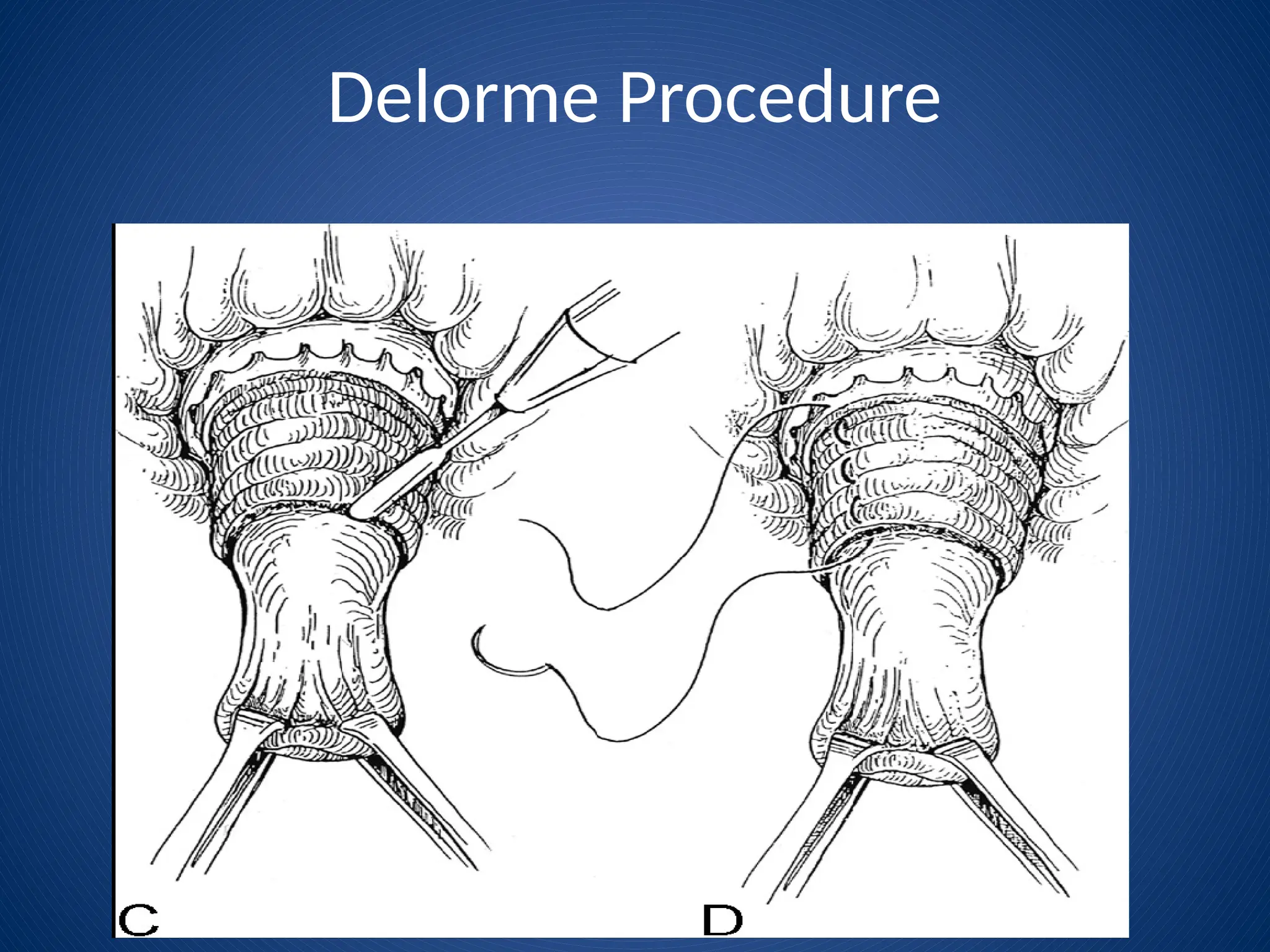
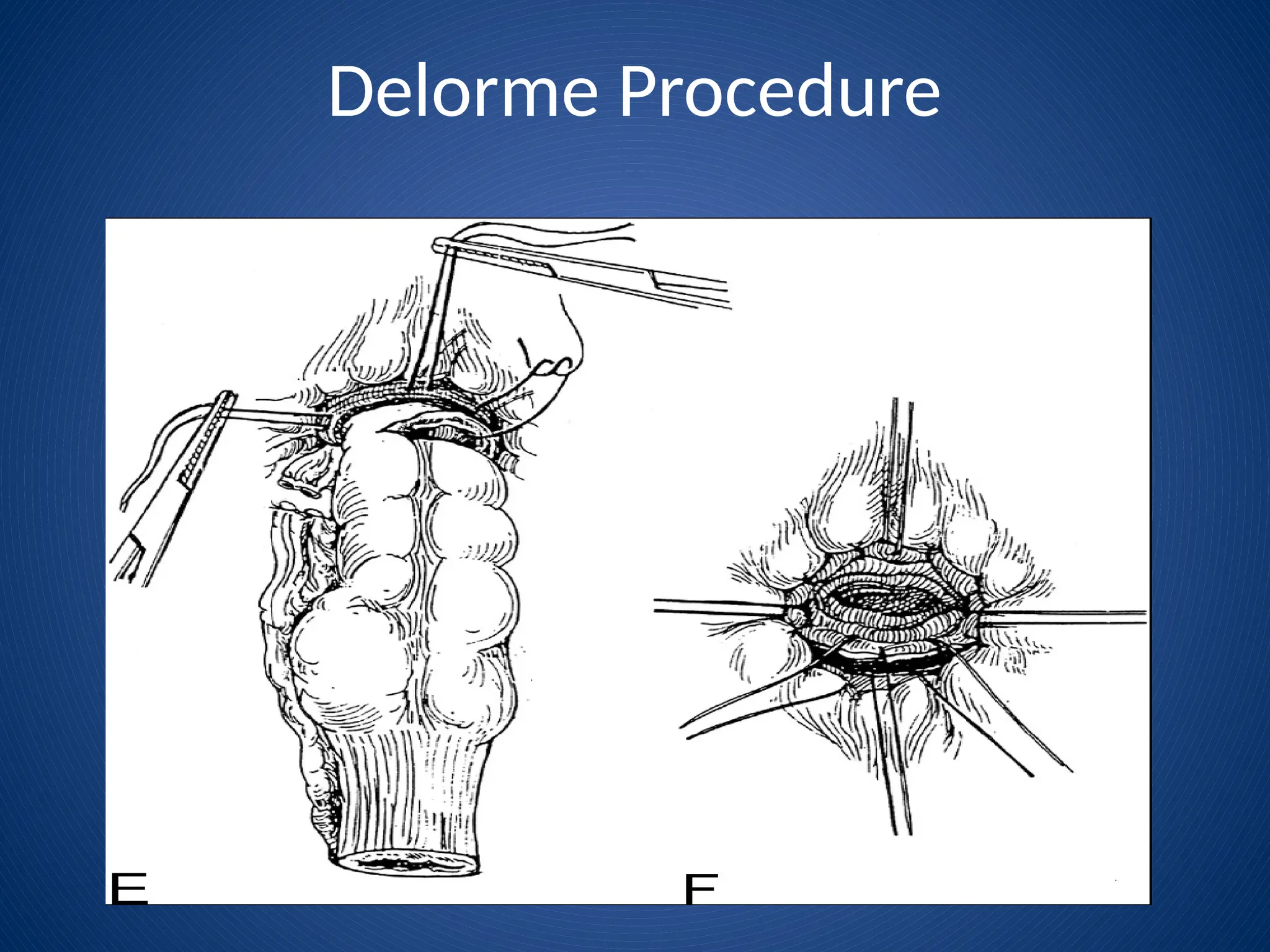
Delorme’s procedure
Onlymucosa and submucosa are excised
Submucosa infiltrated with epine. solution
Mucosa incised 1cm proximal to dentate
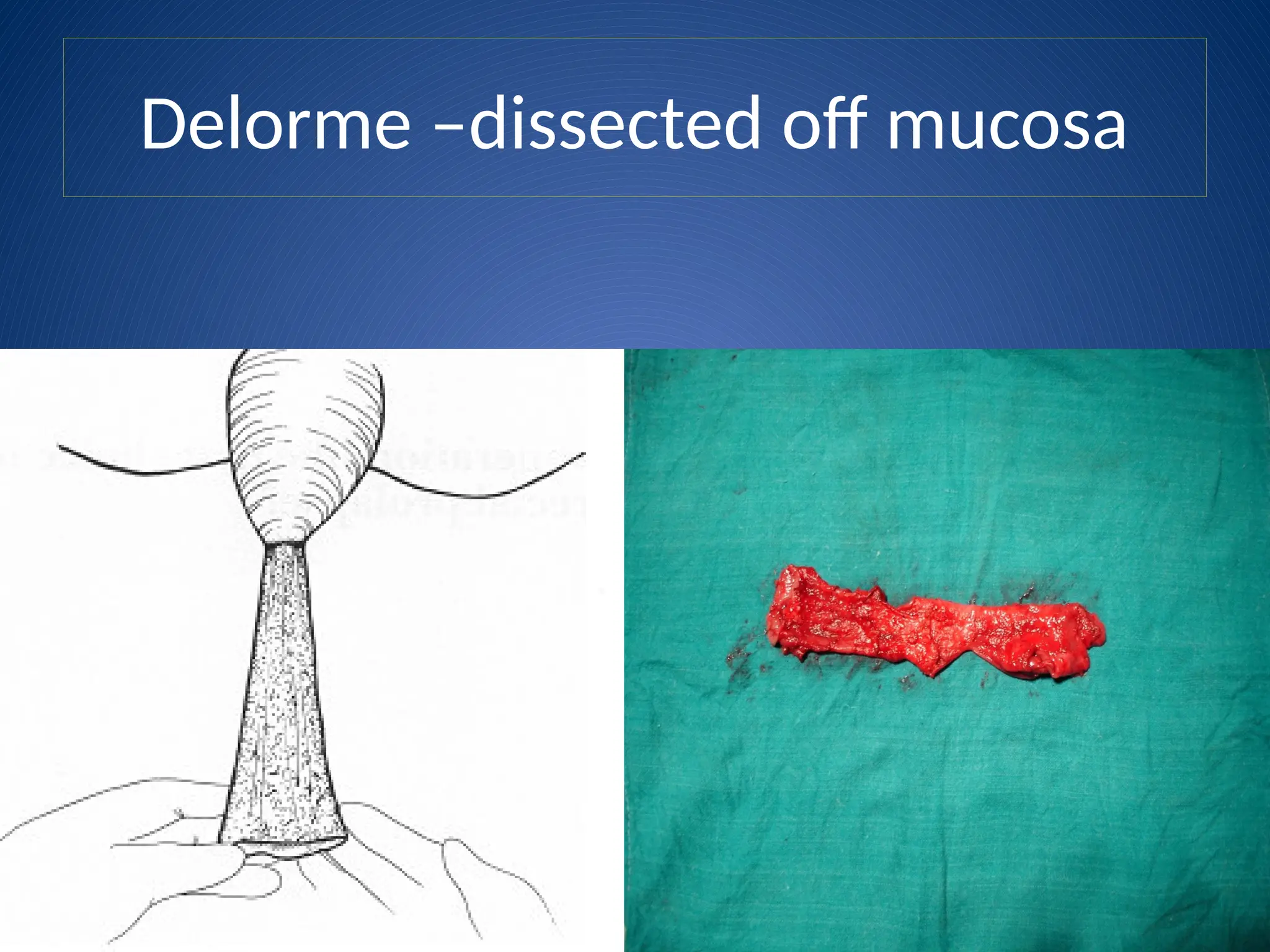
Mucosa and submucosa dissected off underlying
muscle
Continues to apex of prolapse then mucosa
transected
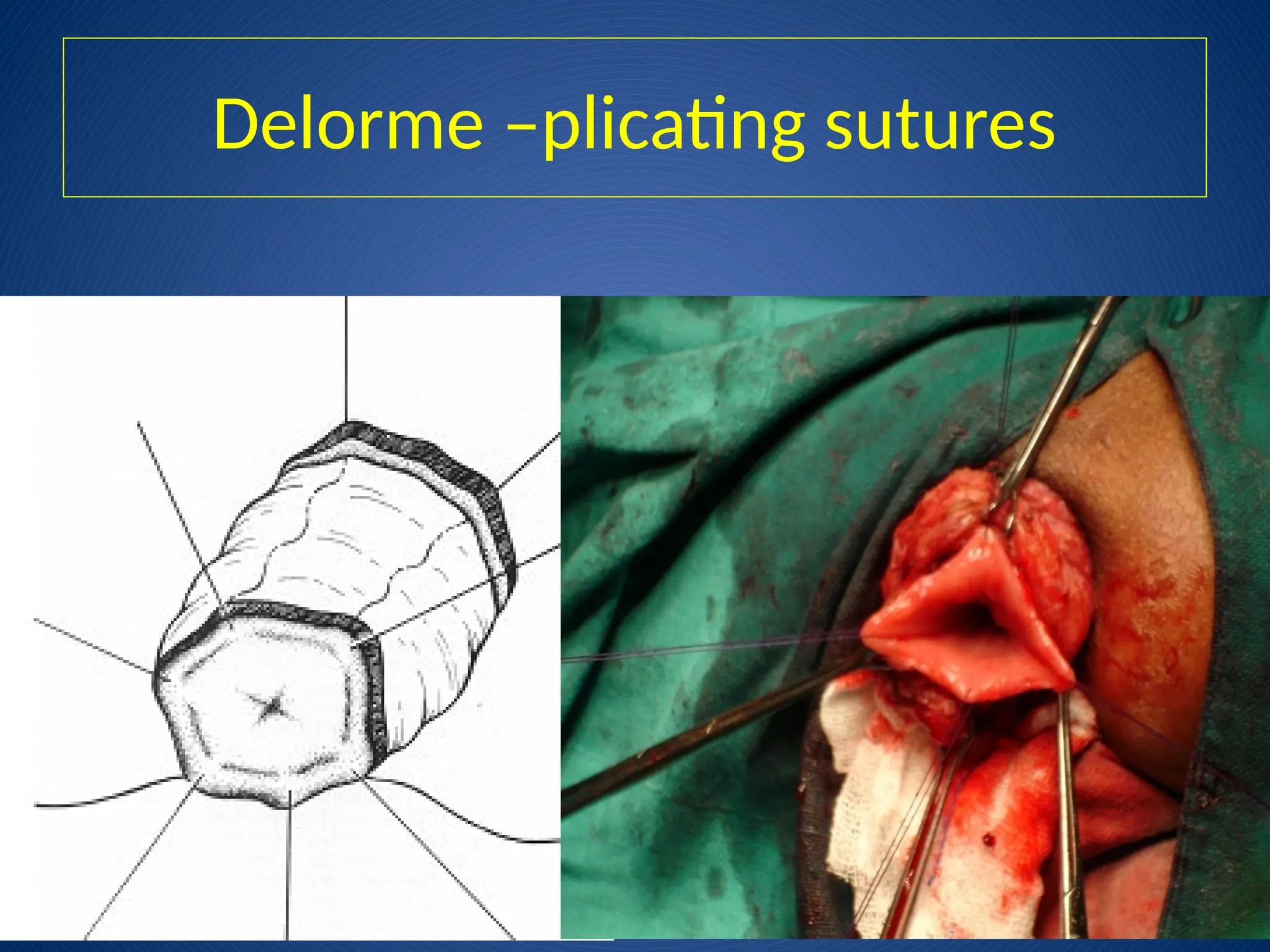
Placating sutures are placed in the muscle
Mucosa is re-approximated
Laparoscopic Rectopexy
♦ Largelyreplacing open abdominal procedures
♦ Ease of performing rectopexy and colon resection
simultaneously with shorter hospital stay
♦ Morbidity and mortality no different than open controls
♦ Recurrence rate lower but not statistically significant
39.
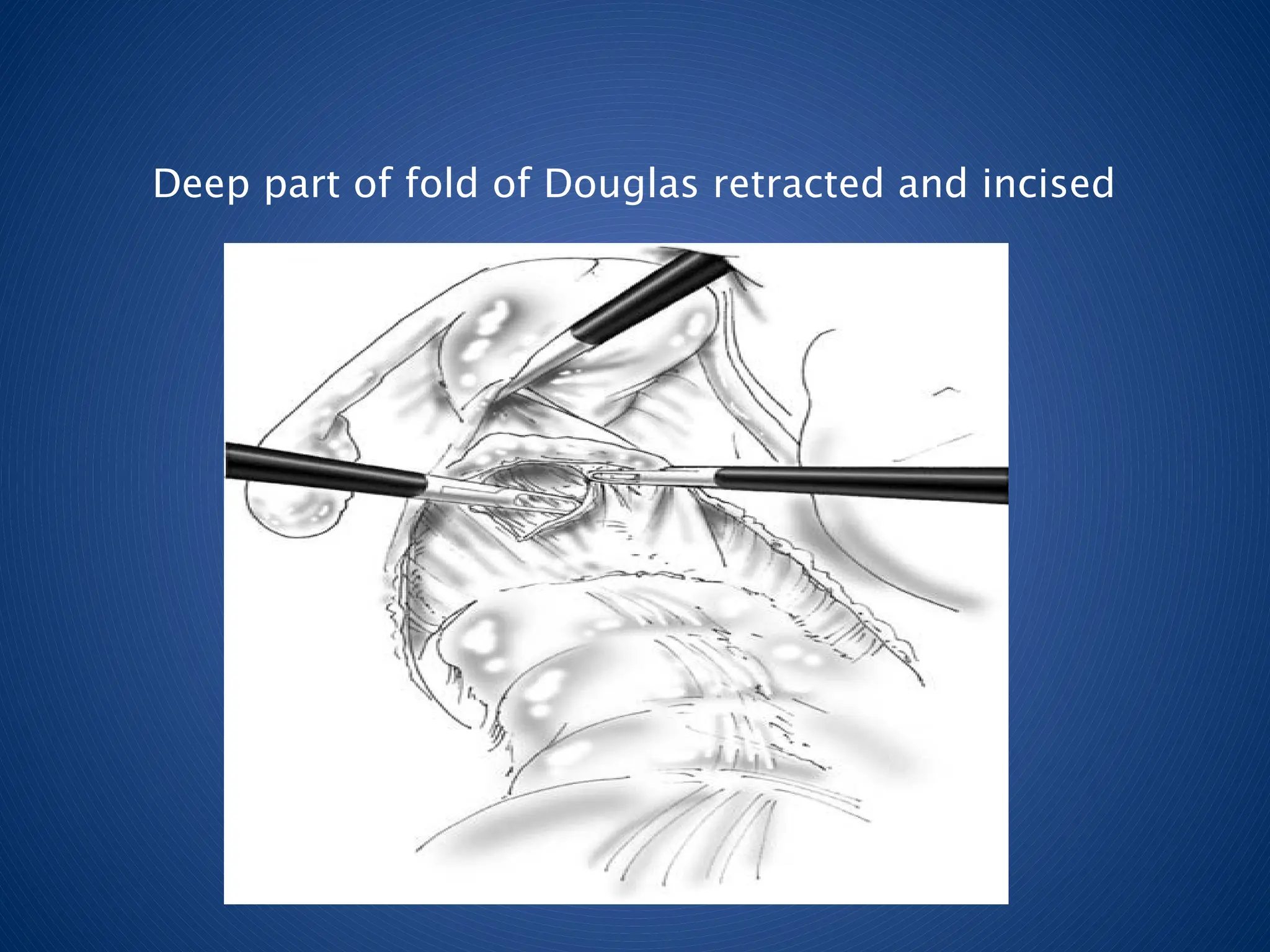
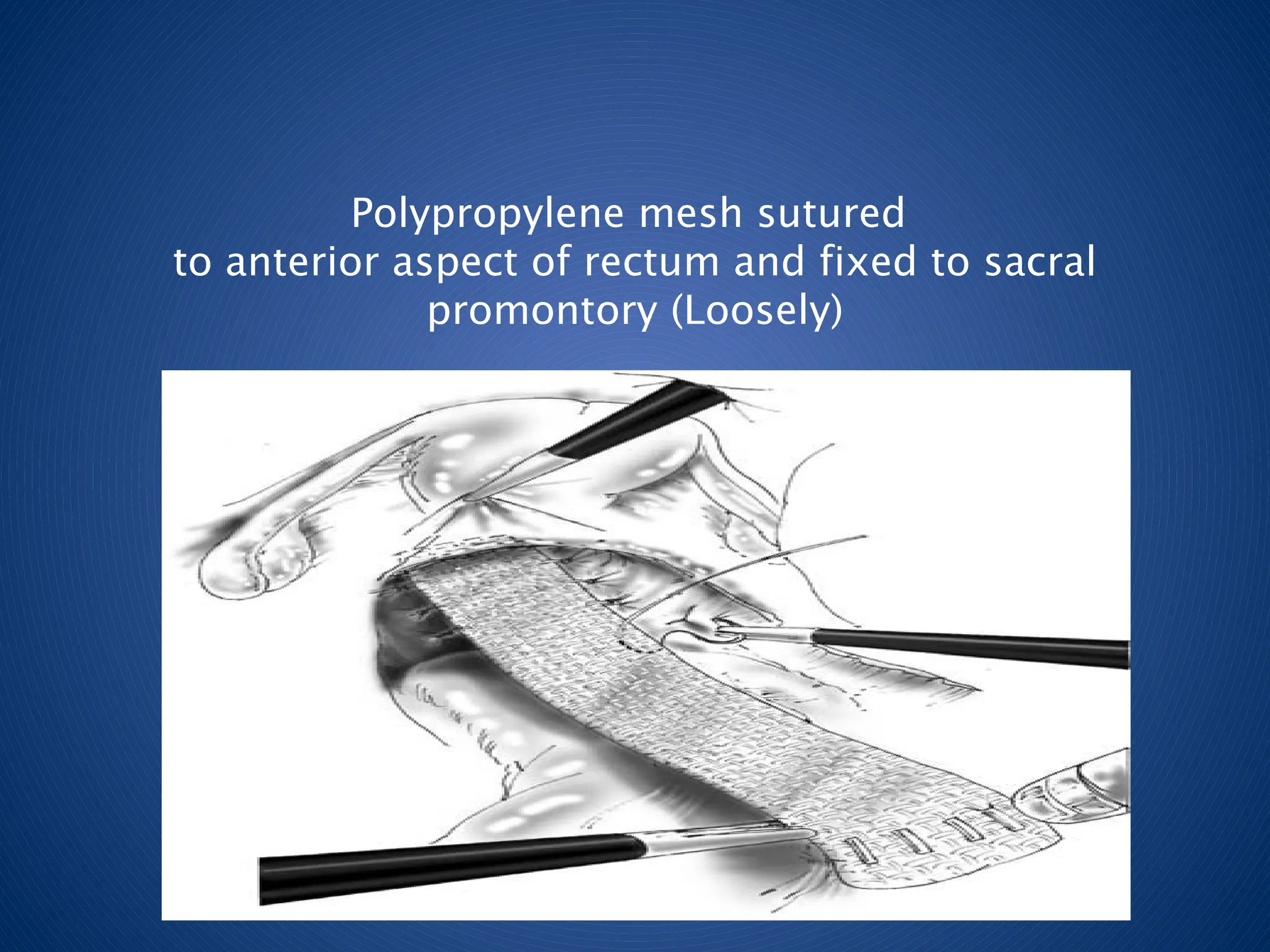
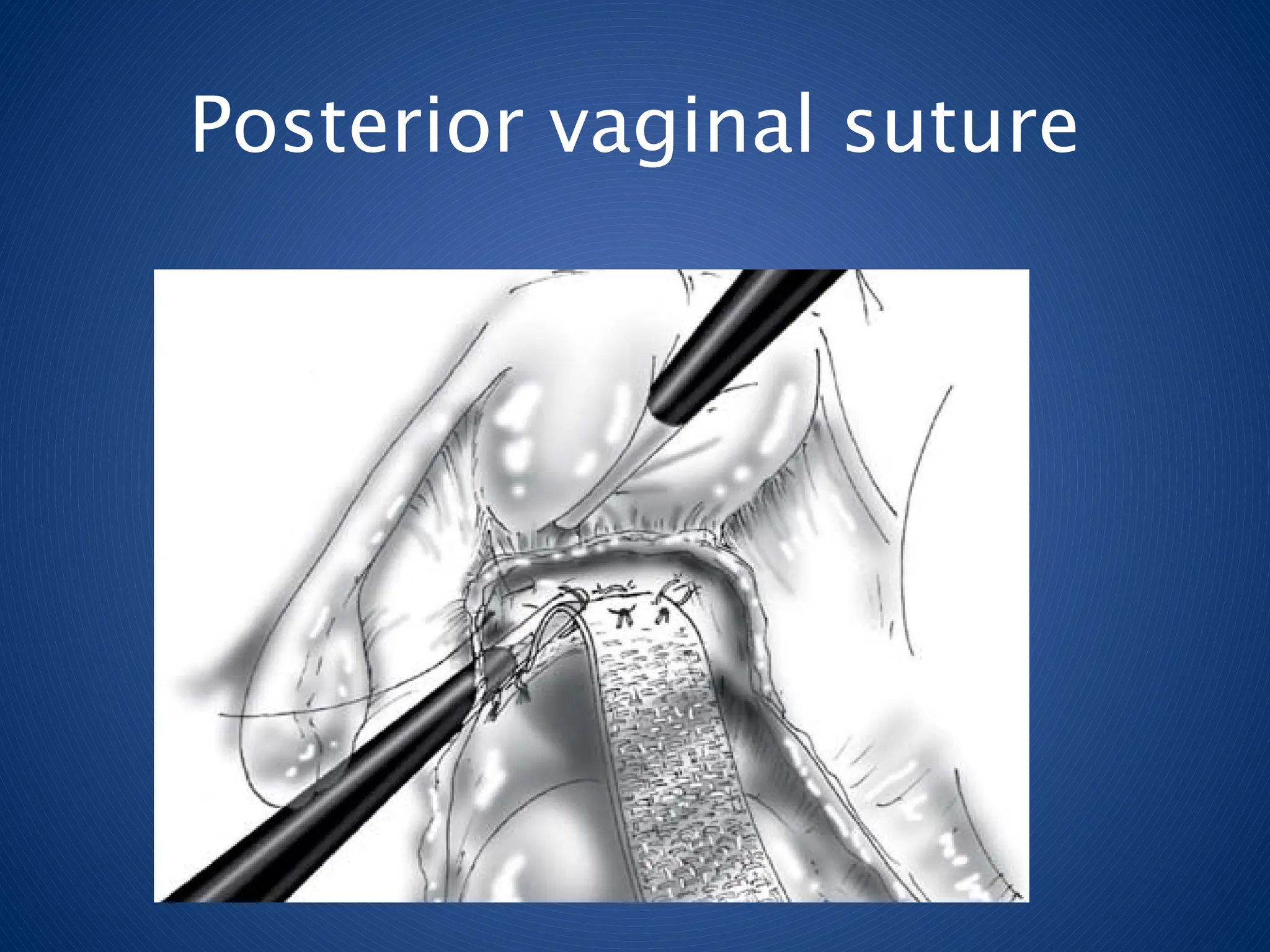
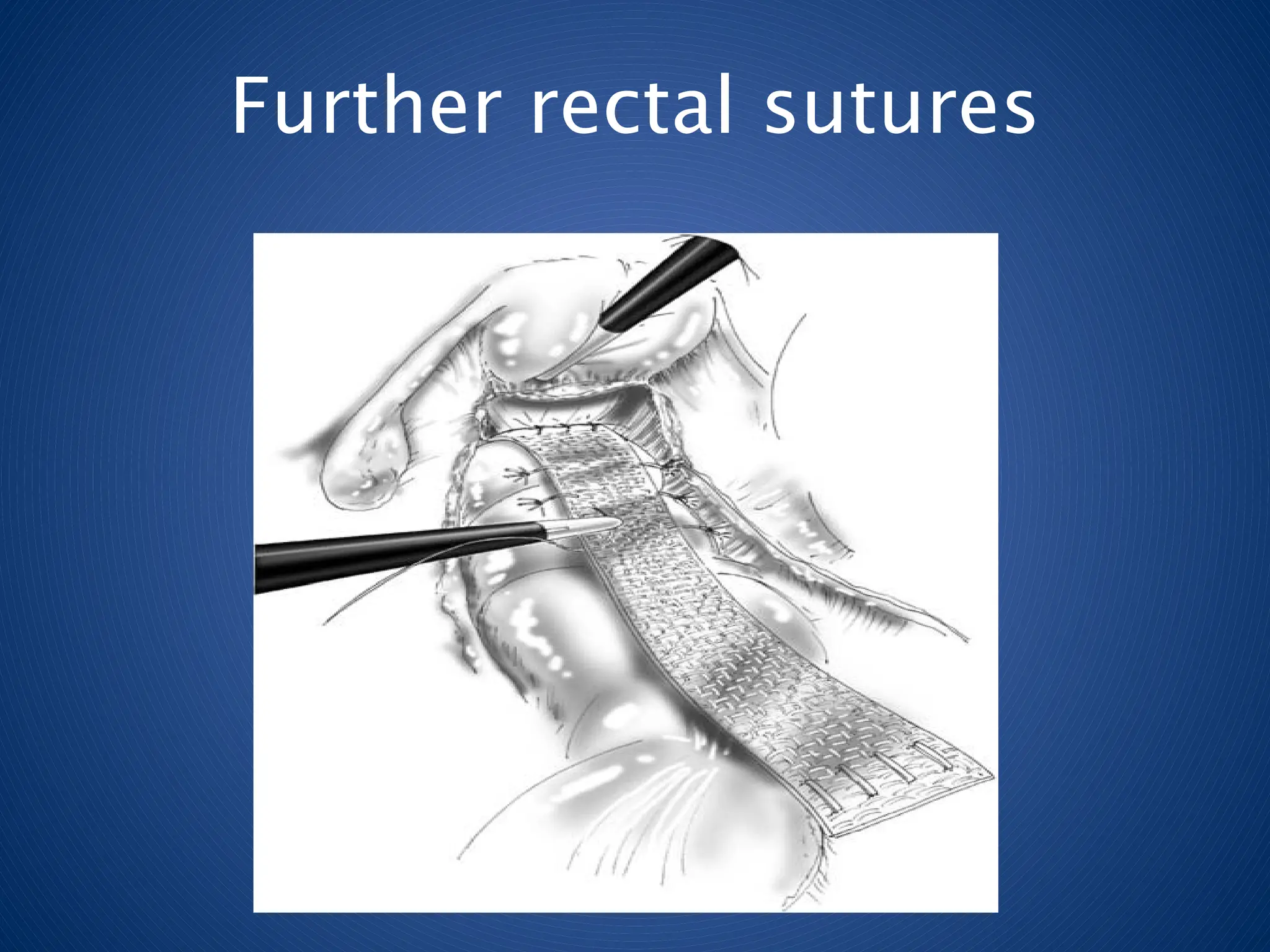
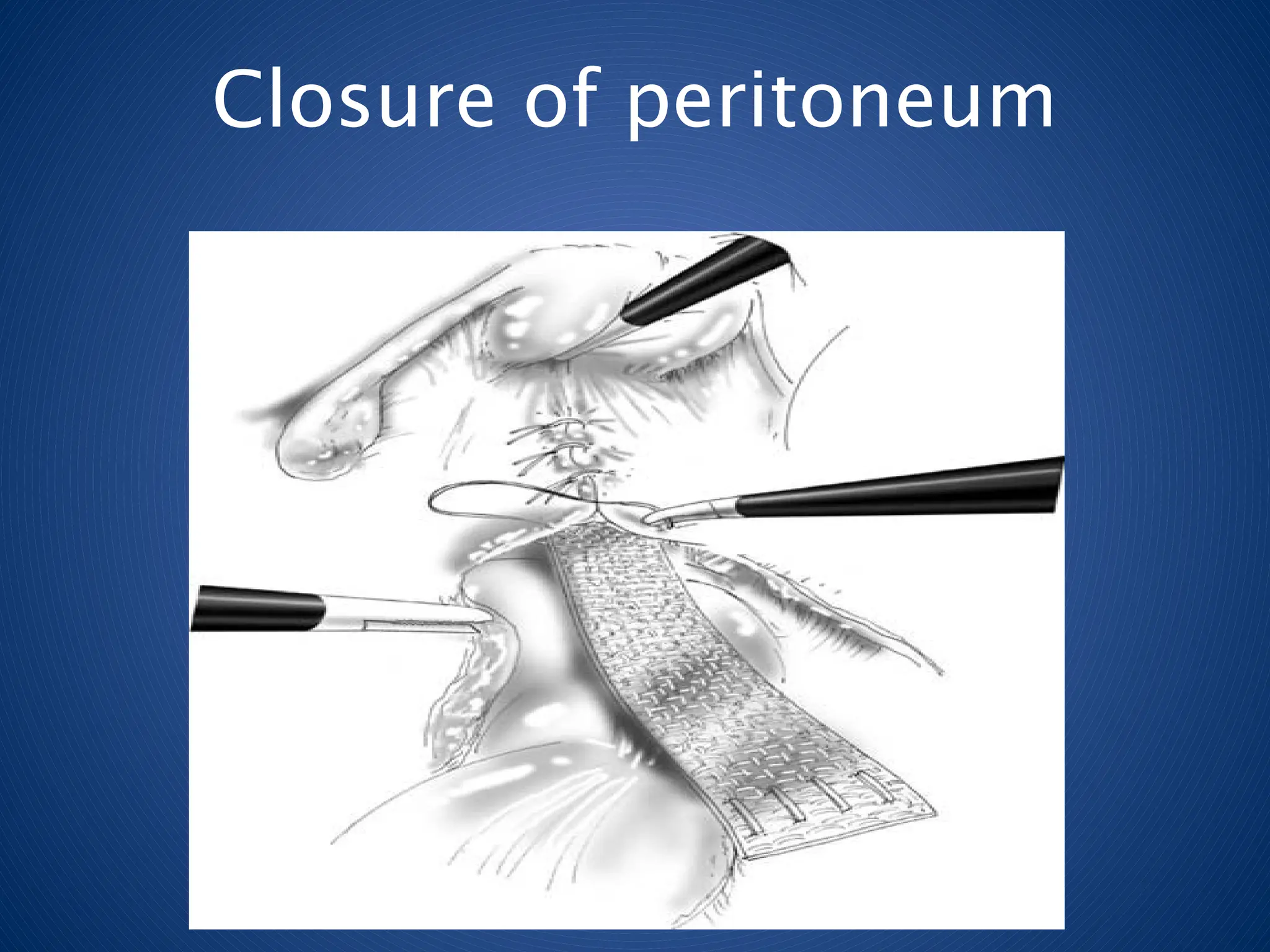
Lap ventral meshRectopexy
• Purpose of surgery : to correct prolapse,
protect or restore continence and avoid
constipation
• Correct middle compartment prolapse
too
Rectopexy +/- Resection
♦Rectopexy with resection - Multiple papers
● Improvement in continence and constipation
● Mortality – 0-6.7%
● Recurrence – 0-5%
♦ Rectopexy without resection - Wilson et. Al
● 9% recurrence at 48 month f/u
● 17% severe constipation managed by laxatives
47.
Conclusions
♦ Consider surgerywhen conservative therapy fails
♦ Careful pt selection is crucial to satisfactory outcome
♦ Tailor surgery to the specific pt
♦ Laparoscopic rectopexy allows for quicker recovery
and shorter LOS but similar recurrence
♦ Regardless of material used, correct suture and tack
placements are crucial
♦ If severely constipated, perform sigmoidectomy
♦ Pts care as much about continence and constipation